

Diverse mechanisms underlying the fetal growth course in gastroschisis and omphalocele
- PMID: 37424955
- PMCID: PMC10329168
- DOI: 10.1016/j.xagr.2023.100238
Diverse mechanisms underlying the fetal growth course in gastroschisis and omphalocele
Abstract
Background: Gastroschisis and omphalocele are the 2 most common congenital fetal abdominal wall defects. Both malformations are commonly associated with small-for-gestational-age neonates. However, the extent and causes of growth restriction remain controversial in both gastroschisis and omphalocele without associated malformations or aneuploidy.
Objective: This study aimed to examine the role of the placenta and the birthweight-to-placental weight ratio in fetuses with abdominal wall defects.
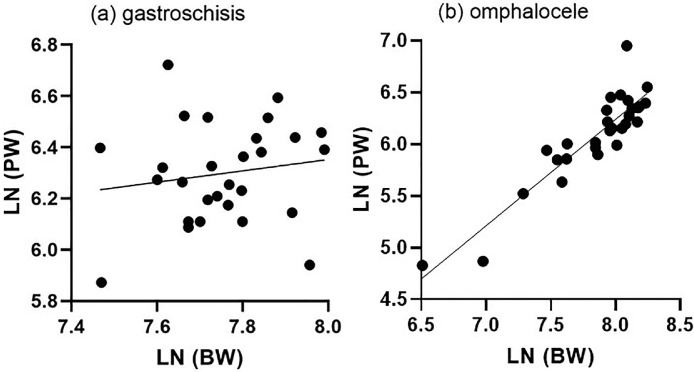
Study design: This study included all cases of abdominal wall defects examined at our hospital between January 2001 and December 2020, retrieving the data from the hospital's software. Fetuses with any other combined congenital anomalies, known chromosomal abnormalities, or lost to follow-up were excluded. Overall, 28 singleton pregnancies with gastroschisis and 24 singleton pregnancies with omphalocele met the inclusion criteria. Patient characteristics and pregnancy outcomes were reviewed. The primary outcome was to investigate the association between birthweight and placental weight in pregnancies with abdominal wall defects as measured after delivery. To correct for gestational age and to compare total placental weights, ratios between the observed and expected birthweights for the given gestational age in singletons were calculated. The scaling exponent β was compared with the reference value of 0.75. Statistical analysis was performed using GraphPad Prism (version 8.2.1; GraphPad Software, San Diego, CA) and IBM SPSS Statistics. A P value of <.05 indicated statistical significance.
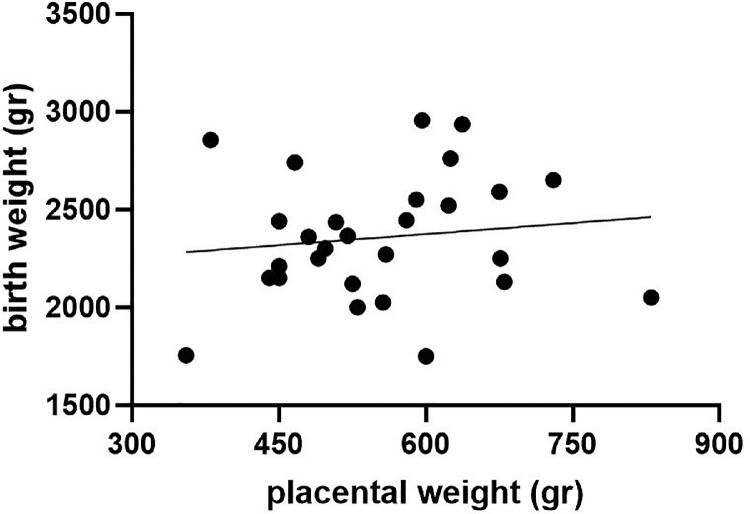
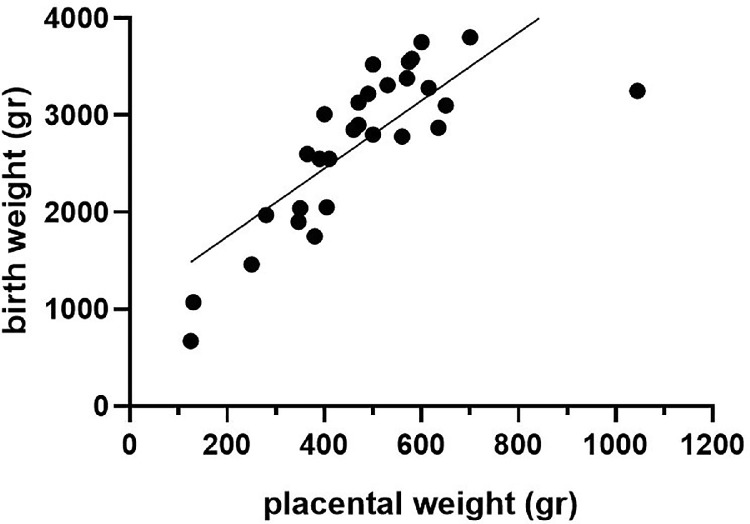
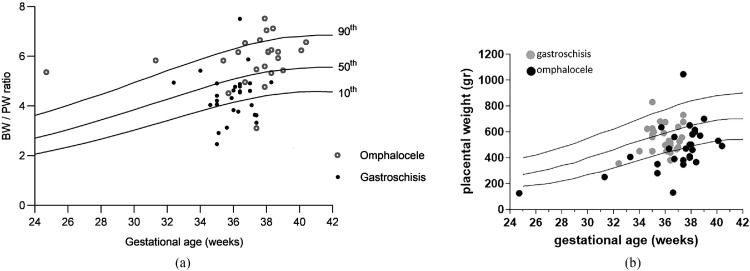
Results: Women pregnant with a fetus with gastroschisis were significantly younger and more often nulliparous. In addition, in this group, the gestational age of delivery was significantly earlier and almost exclusively for cesarean delivery. Of 28 children, 13 (46.7%) were born small for gestational age, only 3 of them (10.7%) had a placental weight <10th percentile. There is no correlation between birthweight percentiles and placental weight percentiles (P=not significant). However, in the omphalocele group, 4 of 24 children (16.7%) were born small for gestational age (<10th percentile), and all children also had a placental weight <10th percentile. There is a significant correlation between birthweight percentiles and placental weight percentiles (P<.0001). The birthweight-to-placental weight ratio differs significantly between pregnancies diagnosed with gastroschisis and pregnancies diagnosed with omphalocele (4.48 [3.79-4.91] vs 6.05 [5.38-6.47], respectively; P<.0001). Allometric metabolic scaling revealed that placentas complicated by gastroschisis and placentas complicated by omphalocele do not scale with birthweight.
Conclusion: Fetuses with gastroschisis displayed impaired intrauterine growth, which seemed to differ from the classical placental insufficiency growth restriction.
Keywords: abdominal wall defects; birthweight; growth restriction; omphalocele and gastroschisis; placental weight.
© 2023 The Authors.
Figures
References
-
- Prefumo F, Izzi C. Fetal abdominal wall defects. Best Pract Res Clin Obstet Gynaecol. 2014;28:391–402. - PubMed
-
- Burton GJ, Jauniaux E. Pathophysiology of placental-derived fetal growth restriction. Am J Obstet Gynecol. 2018;218:S745–S761. - PubMed
-
- Sun C, Groom KM, Oyston C, Chamley LW, Clark AR, James JL. The placenta in fetal growth restriction: what is going wrong? Placenta. 2020;96:10–18. - PubMed
-
- Salavati N, Gordijn SJ, Sovio U, et al. Birth weight to placenta weight ratio and its relationship to ultrasonic measurements, maternal and neonatal morbidity: a prospective cohort study of nulliparous women. Placenta. 2018;63:45–52. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
