

Death, reoperation, and late cardiopulmonary function after truncus repair
- PMID: 37425460
- PMCID: PMC10328806
- DOI: 10.1016/j.xjon.2023.02.010
Death, reoperation, and late cardiopulmonary function after truncus repair
Abstract
Objective: To identify the late surgical outcomes of truncus arteriosus.
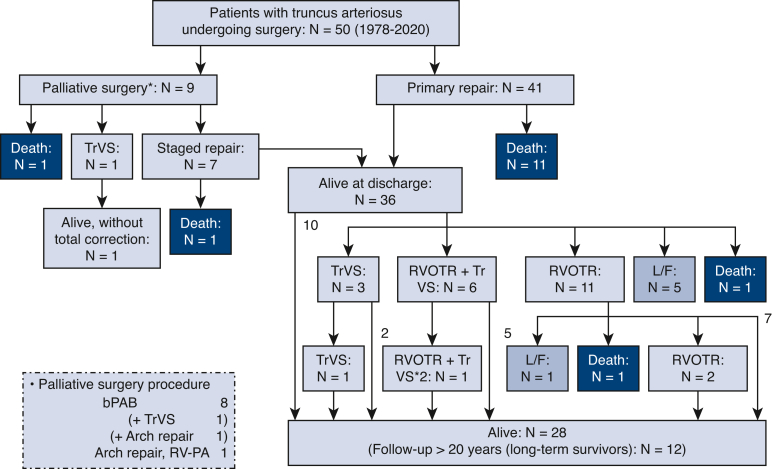
Methods: Fifty consecutive patients with truncus arteriosus who underwent surgery between 1978 and 2020 at our institute were enrolled in this retrospective, single institutional cohort study. The primary outcome was death and reoperation. The secondary outcome was late clinical status, including exercise capacity. The peak oxygen uptake was measured by a ramp-like progressive exercise test on a treadmill.
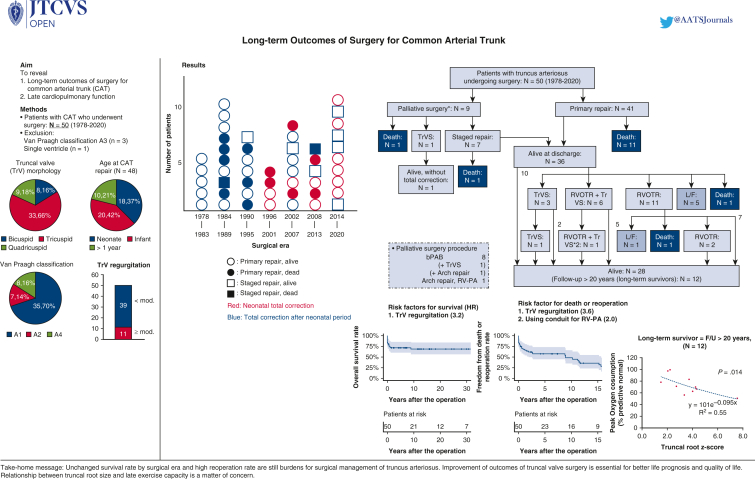
Results: Nine patients underwent palliative surgery, which resulted in 2 deaths. Forty-eight patients went on to truncus arteriosus repair, including 17 neonates (35.4%). The median age and body weight at repair were 92.5 days (interquartile range, 10-272 days) and 3.85 kg (interquartile range, 2.9-6.5 kg), respectively. The survival rate at 30 years was 68.5%. Significant truncal valve regurgitation (P = .030) was a risk factor for survival. Survival rates were similar between in the early 25 and late 25 patients (P = .452). The freedom from death or reoperation rate at 15 years was 35.8%. Significant truncal valve regurgitation was a risk factor (P = .001). The mean follow-up period in hospital survivors was 15.4 ± 12 years (maximum, 43 years). The peak oxygen uptake, which was performed in 12 long-term survivors at a median duration from repair of 19.7 years (interquartile range, 16.8-30.9 years), was 70.2% of predicted normal (interquartile range, 64.5%-80.4%).
Conclusions: Truncal valve regurgitation was a risk factor for both survival and reoperation, thus improvement of truncal valve surgery is essential for better life prognosis and quality of life. Slightly reduced exercise tolerance was common in long-term survivors.
Keywords: truncal root dilatation; truncal valve regurgitation; truncus arteriosus.
© 2023 The Author(s).
Figures





Similar articles
-
Outcomes of Surgical Repair for Persistent Truncus Arteriosus from Neonates to Adults: A Single Center's Experience.PLoS One. 2016 Jan 11;11(1):e0146800. doi: 10.1371/journal.pone.0146800. eCollection 2016. PLoS One. 2016. PMID: 26752522 Free PMC article.
-
Repair of the truncal valve and associated interrupted arch in neonates with truncus arteriosus.J Thorac Cardiovasc Surg. 2000 Mar;119(3):508-14. doi: 10.1016/s0022-5223(00)70130-9. J Thorac Cardiovasc Surg. 2000. PMID: 10694611
-
Long-term follow-up of truncus arteriosus repaired in infancy: a twenty-year experience.J Thorac Cardiovasc Surg. 1997 May;113(5):869-78; discussion 878-9. doi: 10.1016/S0022-5223(97)70259-9. J Thorac Cardiovasc Surg. 1997. PMID: 9159620
-
Surgery for Truncus Arteriosus: Contemporary Practice.Ann Thorac Surg. 2021 May;111(5):1442-1450. doi: 10.1016/j.athoracsur.2020.06.036. Epub 2020 Aug 20. Ann Thorac Surg. 2021. PMID: 32828754 Review.
-
Outcome of truncus arteriosus repair: 20 years of single-center experience comparing early versus late surgical repair.Cardiol Young. 2022 Aug;32(8):1289-1295. doi: 10.1017/S104795112100408X. Epub 2021 Oct 20. Cardiol Young. 2022. PMID: 34666851 Review.
Cited by
-
Systematic Review of the Role of CT Angiocardiography in Enhancing the Diagnosis and Management of Truncus Arteriosus.Med J Islam Repub Iran. 2025 Mar 17;39:41. doi: 10.47176/mjiri.39.41. eCollection 2025. Med J Islam Repub Iran. 2025. PMID: 40740584 Free PMC article. Review.
-
Truncal valve management: The keystone of success.JTCVS Open. 2023 Jul 1;16:810. doi: 10.1016/j.xjon.2023.06.008. eCollection 2023 Dec. JTCVS Open. 2023. PMID: 38204690 Free PMC article. No abstract available.
References
-
- Hoffman J.I., Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol. 2002;39:1890–1900. - PubMed
-
- McGoon D.C., Rastelli G.K., Ongley P.A. An operation for the correction of truncus arteriosus. JAMA. 1968;205:69–73. - PubMed
-
- Hanley F.L., Heinemann M.K., Jonas R.A., Mayer J.E., Jr., Cook N.R., Wessel D.L., et al. Repair of truncus arteriosus in the neonate. J Thorac Cardiovasc Surg. 1993;105:1047–1056. - PubMed
-
- Bove E.L., Lupinetti F.M., Pridjian A.K., Beekman R.H., III, Callow L.B., Snider A.R., et al. Results of a policy of primary repair of truncus arteriosus in the neonate. J Thorac Cardiovasc Surg. 1993;105:1057–1065. - PubMed
LinkOut - more resources
Full Text Sources
