

Racial disparities in surgical treatment of type A acute aortic dissection
- PMID: 37425478
- PMCID: PMC10328814
- DOI: 10.1016/j.xjon.2023.02.002
Racial disparities in surgical treatment of type A acute aortic dissection
Abstract
Objective: To determine whether there are racial disparities associated with mortality, cost, and length of hospital stay after surgical repair of type A acute aortic dissection (TAAAD).
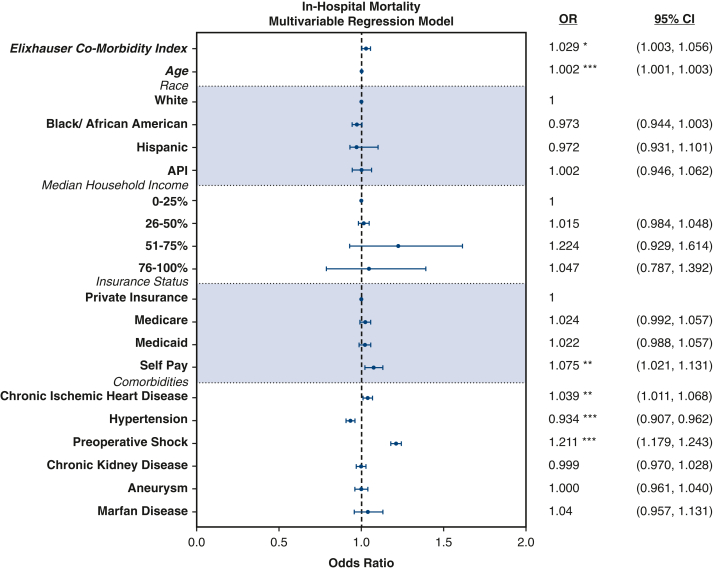
Methods: Patient data from 2015 to 2018 were collected using the National Inpatient Sample. In-hospital mortality was the primary outcome. Multivariable logistical modeling was used to identify factors independently associated with mortality.
Results: Among 3952 admissions, 2520 (63%) were White, 848 (21%) were Black/African American, 310 (8%) were Hispanic, 146 (4%) were Asian and Pacific Islander (API), and 128 (3%) were classified as Other. Black/African American and Hispanic admissions presented with TAAAD at a median age of 54 years and 55 years, respectively, whereas White and API admissions presented at a median age of 64 years and 63 years, respectively (P < .0001). Additionally, there were higher percentages of Black/African American (54%; n = 450) and Hispanic (32%; n = 94) admissions living in ZIP codes with the lowest median household income quartile. Despite these differences on presentation, when adjusting for age and comorbidity, there was no independent association between race and in-hospital mortality and no significant interactions between race and income on in-hospital mortality.
Conclusions: Black and Hispanic admissions present with TAAAD a decade earlier than White and API admissions. Additionally, Black and Hispanic TAAAD admissions are more likely to come from lower-income households. After adjusting for relevant cofactors, there was no independent association between race and in-hospital mortality after surgical treatment of TAAAD.
Keywords: aortic dissection; racial disparities; type A aortic dissection.
© 2023 The Author(s).
Figures






References
-
- Melvinsdottir I.H., Lund S.H., Agnarsson B.A., Sigvaldason K., Gudbjartsson T., Geirsson A. The incidence and mortality of acute thoracic aortic dissection: results from a whole nation study. Eur J Cardio Thorac Surg. 2016;50:1111–1117. - PubMed
-
- Olsson C., Thelin S., Ståhle E., Ekbom A., Granath F. Thoracic aortic aneurysm and dissection: increasing prevalence and improved outcomes reported in a nationwide population-based study of more than 14 000 cases from 1987 to 2002. Circulation. 2006;114:2611–2618. - PubMed
-
- Rylski B., Hoffmann I., Beyersdorf F., Suedkamp M., Siepe M., Nitsch B., et al. Acute aortic dissection type A: age-related management and outcomes reported in the German Registry for Acute Aortic Dissection Type A (GERAADA) of over 2000 patients. Ann Surg. 2014;259:598–604. - PubMed
-
- Zimmerman K.P., Oderich G., Pochettino A., Hanson K.T., Habermann E.B., Bower T.C., et al. Improving mortality trends for hospitalization of aortic dissection in the National Inpatient Sample. J Vasc Surg. 2016;64:606–615.e1. - PubMed
LinkOut - more resources
Full Text Sources
