

Development of prognostic models to estimate the probability of lung injury one year after COVID-19-related hospitalization-a prospective study
- PMID: 37426134
- PMCID: PMC10323564
- DOI: 10.21037/jtd-22-1565
Development of prognostic models to estimate the probability of lung injury one year after COVID-19-related hospitalization-a prospective study
Abstract
Background: Long-term effects of severe acute respiratory syndrome coronavirus 2 (SARS-COV-2) infection still under study. The objectives of this study were to identify persistent pulmonary lesions 1 year after coronavirus disease 2019 (COVID-19) hospitalization and assess whether it is possible to estimate the probability that a patient develops these complications in the future.
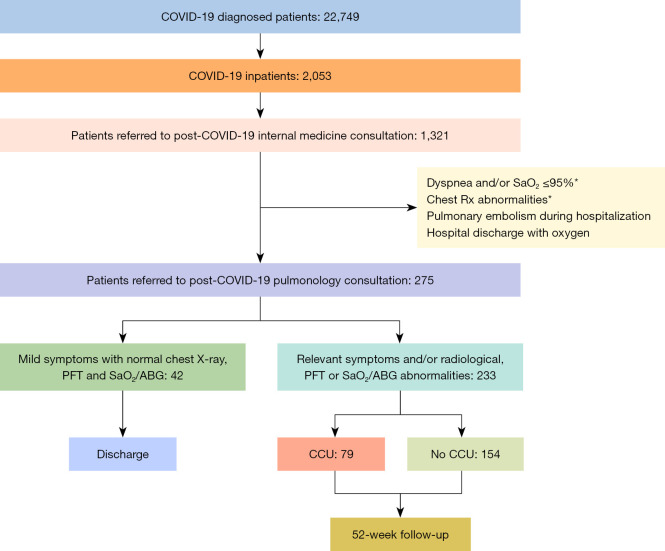
Methods: A prospective study of ≥18 years old patients hospitalized for SARS-COV-2 infection who develop persistent respiratory symptoms, lung function abnormalities or have radiological findings 6-8 weeks after hospital discharge. Logistic regression models were used to identify prognostic factors associated with a higher risk of developing respiratory problems. Models performance was assessed in terms of calibration and discrimination.
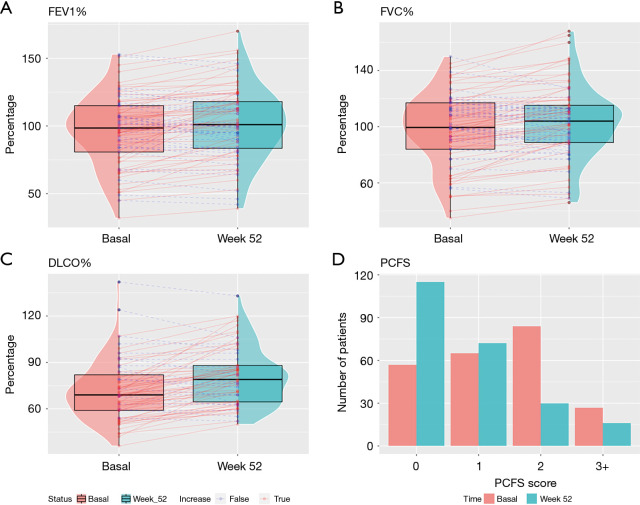
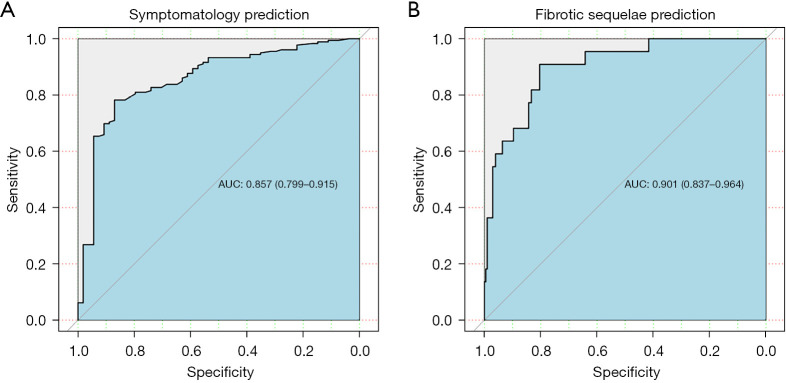
Results: A total of 233 patients [median age 66 years [interquartile range (IQR): 56, 74]; 138 (59.2%) male] were categorized into two groups based on whether they stayed in the critical care unit (79 cases) or not (154). At the end of follow-up, 179 patients (76.8%) developed persistent respiratory symptoms, and 22 patients (9.4%) showed radiological fibrotic lesions with pulmonary function abnormalities (post-COVID-19 fibrotic pulmonary lesions). Our prognostic models created to predict persistent respiratory symptoms [post-COVID-19 functional status at initial visit (the higher the score, the higher the risk), and history of bronchial asthma] and post-COVID-19 fibrotic pulmonary lesions [female; FVC% (the higher the FVC%, the lower the probability); and critical care unit stay] one year after infection showed good (AUC 0.857; 95% CI: 0.799-0.915) and excellent performance (AUC 0.901; 95% CI: 0.837-0.964), respectively.
Conclusions: Constructed models show good performance in identifying patients at risk of developing lung injury one year after COVID-19-related hospitalization.
Keywords: Post-acute coronavirus disease 2019 syndrome (post-acute COVID-19 syndrome); clinical prediction models; fibrotic pulmonary lesions; radiological findings; respiratory functional test; respiratory symptoms.
2023 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-22-1565/coif). The authors have no conflicts of interest to declare.
Figures

References
-
- World Health Organization 2022. Available online: https://covid19.who.int. [Last accessed on 2022 July 10].
LinkOut - more resources
Full Text Sources
Miscellaneous