

Evidence-based opioid prescribing guidelines after lung resection: a prospective, multicenter analysis
- PMID: 37426143
- PMCID: PMC10323572
- DOI: 10.21037/jtd-22-1621
Evidence-based opioid prescribing guidelines after lung resection: a prospective, multicenter analysis
Abstract
Background: Opioid prescribing guidelines have significantly decreased overprescribing and post-discharge use after cardiac surgery; however, limited recommendations exist for general thoracic surgery patients, a similarly high-risk population. We examined opioid prescribing and patient-reported use to develop evidence-based, opioid prescribing guidelines after lung cancer resection.
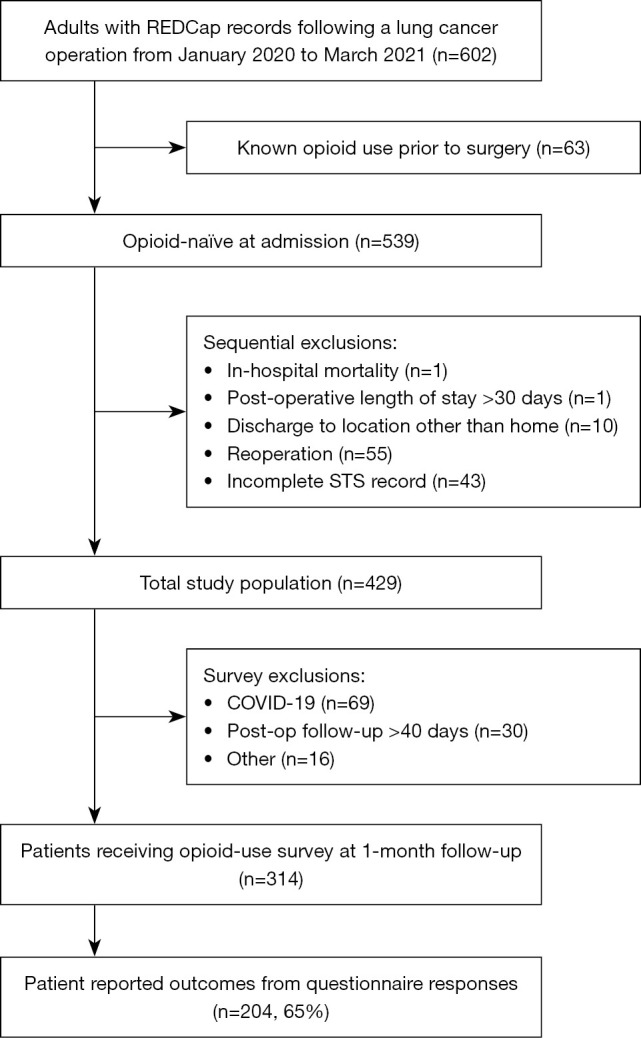
Methods: This prospective, statewide, quality improvement study was conducted between January 2020 to March 2021 and included patients undergoing surgical resection of a primary lung cancer across 11 institutions. Patient-reported outcomes at 1-month follow-up were linked with clinical data and Society of Thoracic Surgery (STS) database records to characterize prescribing patterns and post-discharge use. The primary outcome was quantity of opioid used after discharge; secondary outcomes included quantity of opioid prescribed at discharge and patient-reported pain scores. Opioid quantities are reported in number of 5-mg oxycodone tablets (mean ± standard deviation).
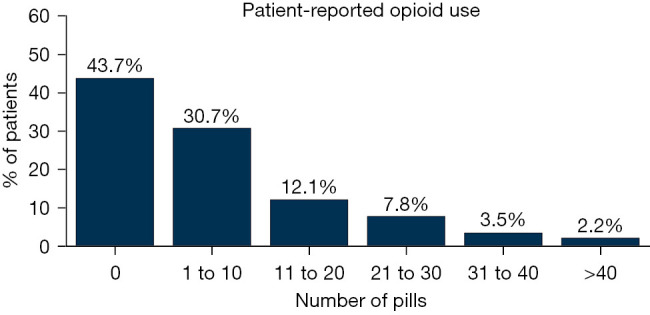
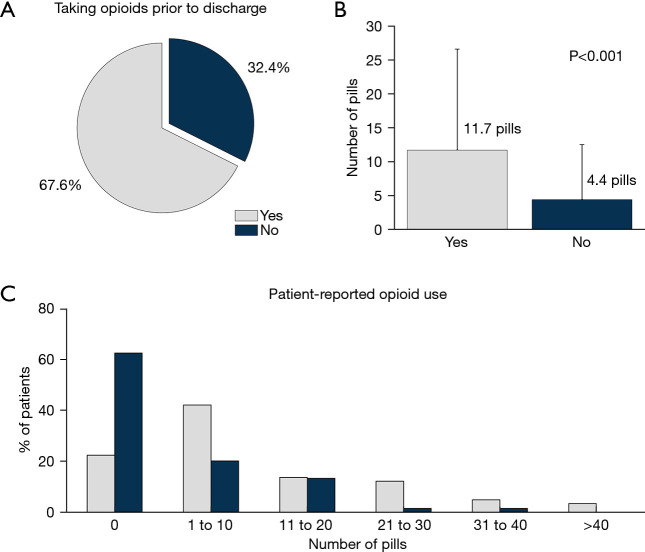
Results: Of the 602 patients identified, 429 met inclusion criteria. Questionnaire response rate was 65.0%. At discharge, 83.4% of patients were provided a prescription for opioids of mean size 20.5±13.1 pills, while patients reported using 8.2±13.0 pills after discharge (P<0.001), including 43.7% who used none. Those not taking opioids on the calendar day prior to discharge (32.4%) used fewer pills (4.4±8.1 vs. 11.7±14.9, P<0.001). Refill rate was 21.5% for patients provided a prescription at discharge, while 12.5% of patients not prescribed opioids at discharge required a new prescription before follow-up. Pain scores were 2.4±2.5 for incision site and 3.0±2.8 for overall pain (scale 0-10).
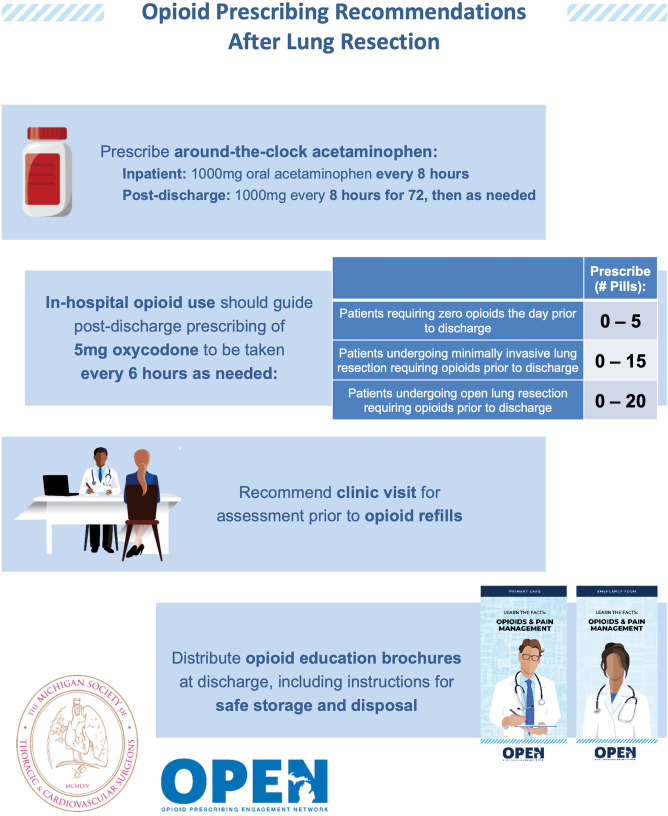
Conclusions: Patient-reported post-discharge opioid use, surgical approach, and in-hospital opioid use before discharge should be used to inform prescribing recommendations after lung resection.
Keywords: Opioid prescribing; lung cancer; practice guidelines; thoracic surgery.
2023 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-22-1621/coif). RMA reports grants and travel expenses when proctoring for Edwards Lifesciences, Intuitive Surgical, and Ethicon – Johnson & Johnson. JR Martin reports consulting fees and webinars for Terumo. CMB reports consulting fees from Heron Therapeutics, Vertex Pharmaceuticals, Benter Foundation, and Alosa Health, as well as receiving payment for providing expert testimony. ACC previously served as the President of the Michigan Society of Thoracic & Cardiovascular Surgeons. The other authors have no conflicts of interest to declare.
Figures
Comment in
-
Opioid prescription guideline is important to enhanced recovery after thoracic surgery protocol.J Thorac Dis. 2023 Oct 31;15(10):5275-5277. doi: 10.21037/jtd-23-1208. Epub 2023 Sep 6. J Thorac Dis. 2023. PMID: 37969260 Free PMC article. No abstract available.
References
LinkOut - more resources
Full Text Sources
Miscellaneous