

Radiation and Dose-densification of R-CHOP in Primary Mediastinal B-cell Lymphoma: Subgroup Analysis of the UNFOLDER Trial
- PMID: 37427145
- PMCID: PMC10325764
- DOI: 10.1097/HS9.0000000000000917
Radiation and Dose-densification of R-CHOP in Primary Mediastinal B-cell Lymphoma: Subgroup Analysis of the UNFOLDER Trial
Abstract
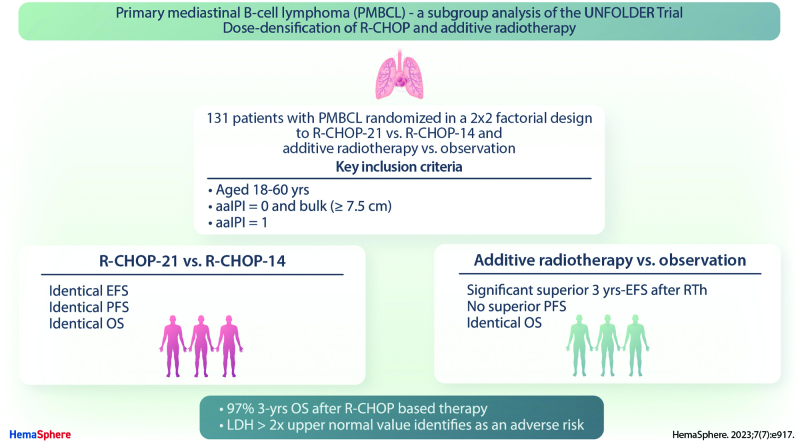
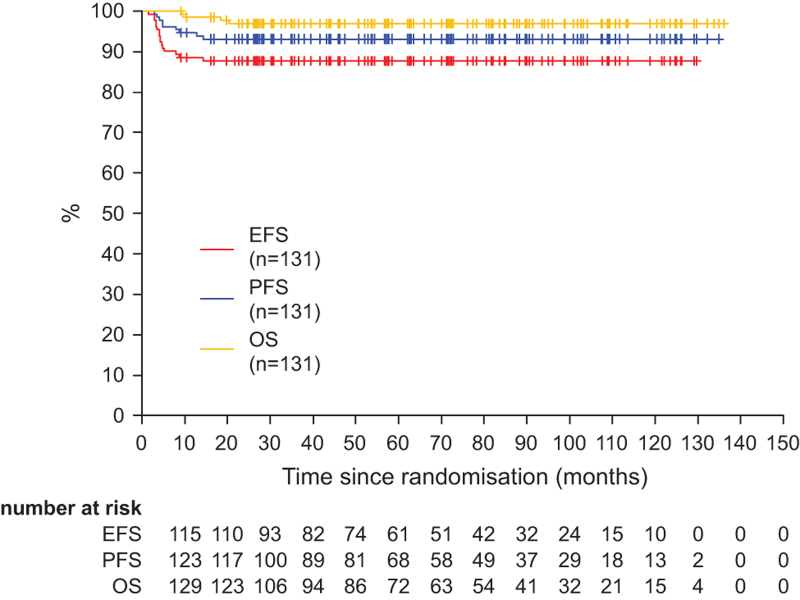
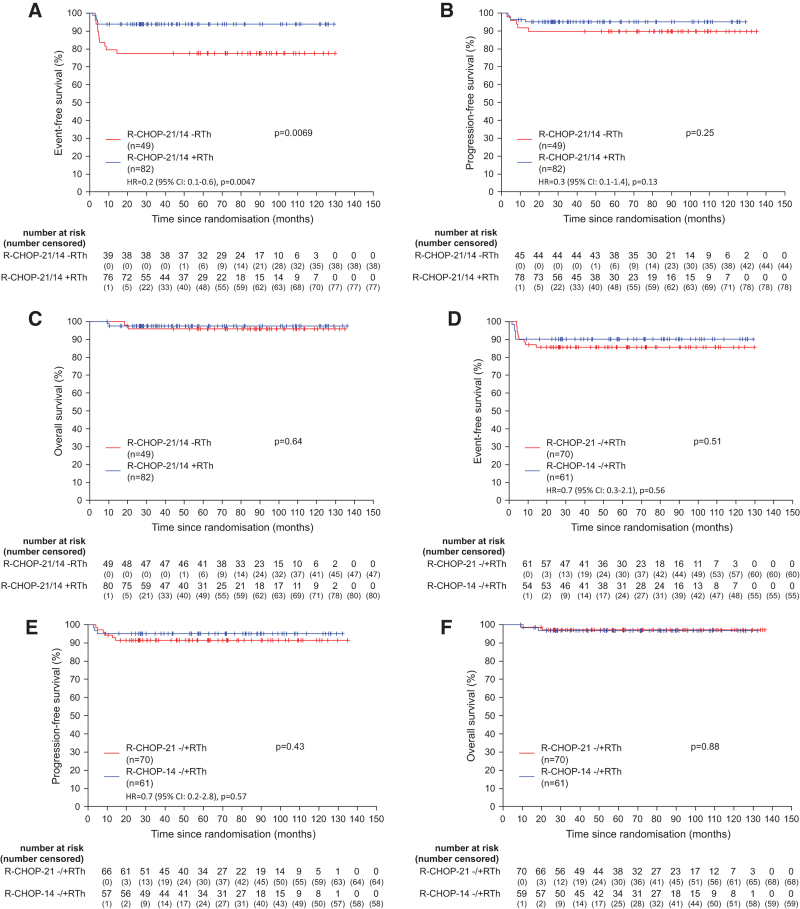
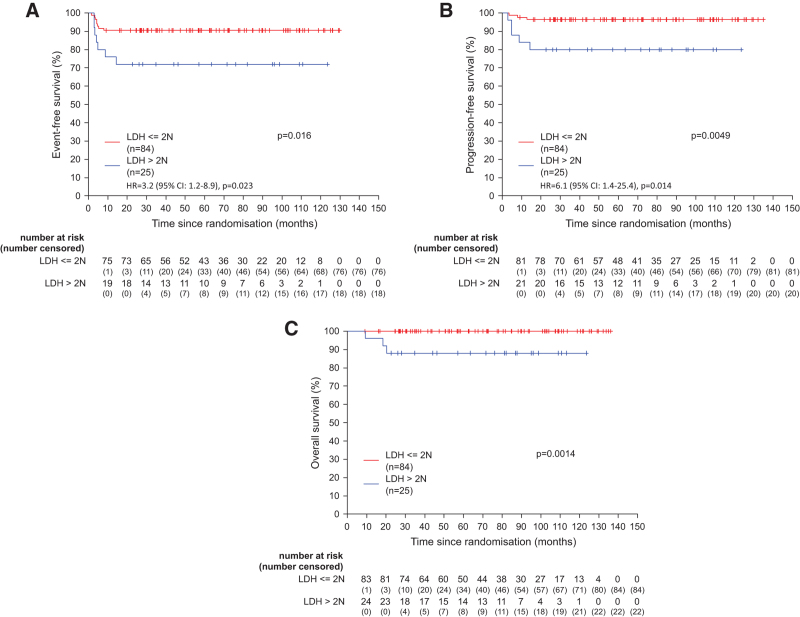
UNFOLDER (NCT00278408, EUDRACT 2005-005218-19) is a phase-3 trial in patients with aggressive B-cell lymphoma and intermediate prognosis, including primary mediastinal B-cell lymphoma (PMBCL). In a 2 × 2 factorial design, patients were randomized to 6× R-CHOP-14 or R-CHOP-21 (rituximab, cyclophosphamide, doxorubicin, vincristine, and prediso(lo)ne) and to consolidation radiotherapy to extralymphatic/bulky disease or observation. Response was assessed according to the standardized criteria from 1999, which did not include F-18 fluordesoxyglucose positron emission tomography/computed tomography (FDG-PET) scans. Primary end point was event-free survival (EFS). A subgroup of 131 patients with PMBCLs was included (median age, 34 y; 54% female, 79% elevated lactate dehydrogenase (LDH), 20% LDH >2× upper limit of normal [ULN], and 24% extralymphatic involvement). Eighty-two (R-CHOP-21: 43 and R-CHOP-14: 39) patients were assigned to radiotherapy and 49 (R-CHOP-21: 27, R-CHOP-14: 22) to observation. The 3-year EFS was superior in radiotherapy arm (94% [95% confidence interval (CI), 89-99] versus 78% [95% CI, 66-89]; P = 0.0069), due to a lower rate of partial responses (PRs) (2% versus 10%). PR triggered additional treatment, mostly radiotherapy (n = 5; PR: 4; complete response/unconfirmed complete response: 1). No significant differences were observed in progression-free survival (PFS) (95% [95% CI, 90-100] versus 90% [95% CI, 81-98]; P = 0.25) nor in overall survival (OS) (98% [95% CI, 94-100] versus 96% [95% CI, 90-100]; P = 0.64). Comparing R-CHOP-14 and R-CHOP-21, EFS, PFS, and OS were not different. A prognostic marker for adverse outcome was elevated LDH >2× ULN (EFS: P = 0.016; PFS: P = 0.0049; OS: P = 0.0014). With the limitation of a pre-PET-era trial, the results suggest a benefit of radiotherapy only for patients responding to R-CHOP with PR. PMBCL treated with R-CHOP have a favorable prognosis with a 3-year OS of 97%.
Copyright © 2023 the Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the European Hematology Association.
Conflict of interest statement
GH has received grants from Roche and Bristol-Myers Squibb and personal fees from Bristol-Myers Squibb, Roche, Amgen, Spectrum and MSD. L Thurner has received travel grants from Abbvie, Janssen and EUSA-Pharm, and has indicated consultancy for Takeda, Astra-Zeneca, Merck, EUSA-pharm. VP has received grants from Deutsche Krebshilfe (German Cancer Aid), Chugai, Abbvie, Amgen, Roche, and Bristol-Myers Squibb. AV has received honoraria from Roche, Amgen, Kite, Gilead, Novartis, Bristol-Myers Squibb and has indicated a membership of the advisory board of Roche, Amgen, Kite, Gilead, Novartis, Bristol-Myers Squibb. MN has received travel grants from Roche, Celgene, and MSD and personal fees from Roche, Celgene, MSD, Janssen, Amgen, Incyte, and Abbvie. FG participates in advisory board of Roche, Boehringer Ingelheim, Abbvie, Merck, Takeda, MSD, Sanofi, Pfizer, Novartis, Amgen, and Janssen. PdNB has indicated consultancy for Roche, Incyte, and Novartis. SS has received grants from Abbvie, Astra-Zeneca, Celgene, Gilead, Roche, Janssen, Novartis, Morphosys and has indicated consultancy for for Abbvie, Astra-Zeneca, Celgene, Gilead, Roche, Janssen, Novartis, Morphosys; he has received drug/equipment supplied by entity from Abbvie, Astra-Zeneca, Celgene, Gilead, Roche, Janssen, Novartis, Morphosys. All the other authors have no conflicts of interest to disclose.
Figures
References
-
- Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. Vol. 2. 4th ed. International Agency for Research on Cancer (IARC); 2017.
-
- Zinzani PL, Martelli M, Bertini M, et al. Induction chemotherapy strategies for primary mediastinal large B-cell lymphoma with sclerosis: a retrospective multinational study on 426 previously untreated patients. Haematologica. 2002;87:1258–1264. - PubMed
-
- Rieger M, Österborg A, Pettengell R, et al. Primary mediastinal B-cell lymphoma treated with CHOP-like chemotherapy with or without rituximab: results of the Mabthera International Trial Group study. Ann Oncol. 2011;22:664–670. - PubMed
-
- Gleeson M, Hawkes EA, Cunningham D, et al. Rituximab, cyclophosphamide, doxorubicin, vincristine and prednisolone (R-CHOP) in the management of primary mediastinal B-cell lymphoma: a subgroup analysis of the UK NCRI R-CHOP 14 versus 21 trial. Br J Haematol. 2016;175:668–672. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous