

Management of covert brain infarction survey: A call to care for and trial this neglected population
- PMID: 37427426
- PMCID: PMC10683731
- DOI: 10.1177/23969873231187444
Management of covert brain infarction survey: A call to care for and trial this neglected population
Abstract
Background: Covert brain infarction (CBI) is highly prevalent and linked with stroke risk factors, increased mortality, and morbidity. Evidence to guide management is sparse. We sought to gain information on current practice and attitudes toward CBI and to compare differences in management according to CBI phenotype.
Methods: We conducted a web-based, structured, international survey from November 2021 to February 2022 among neurologists and neuroradiologists. The survey captured respondents' baseline characteristics, general approach toward CBI and included two case scenarios designed to evaluate management decisions taken upon incidental detection of an embolic-phenotype and a small-vessel-disease phenotype.
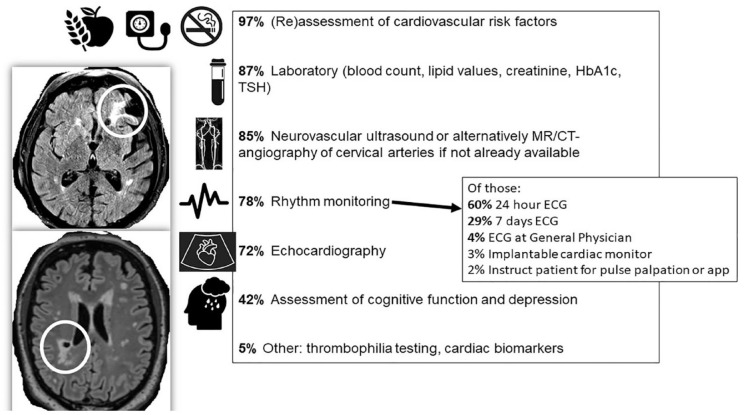
Results: Of 627 respondents (38% vascular neurologists, 24% general neurologists, and 26% neuroradiologists), 362 (58%) had a partial, and 305 (49%) a complete response. Most respondents were university hospital senior faculty members experienced in stroke, mostly from Europe and Asia. Only 66 (18%) of respondents had established institutional written protocols to manage CBI. The majority indicated that they were uncertain regarding useful investigations and further management of CBI patients (median 67 on a slider 0-100, 95% CI 35-81). Almost all respondents (97%) indicated that they would assess vascular risk factors. Although most would investigate and treat similarly to ischemic stroke for both phenotypes, including initiating antithrombotic treatment, there was considerable diagnostic and therapeutic heterogeneity. Less than half of respondents (42%) would assess cognitive function or depression.
Conclusions: There is a high degree of uncertainty and heterogeneity regarding management of two common types of CBI, even among experienced stroke physicians. Respondents were more proactive regarding the diagnostic and therapeutic management than the minimum recommended by current expert opinions. More data are required to guide management of CBI; meantime, more consistent approaches to identification and consistent application of current knowledge, that also consider cognition and mood, would be promising first steps to improve consistency of care.
Keywords: Covert brain infarction; covert cerebrovascular disease; silent brain infarction; silent cerebrovascular disease; survey.
© European Stroke Organisation 2023.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Vernooij MW, Ikram MA, Tanghe HL, et al.. Incidental findings on brain MRI in the general population. N Engl J Med 2007; 357: 1821–1828. - PubMed
-
- Vermeer SE, Longstreth WT, Jr, Koudstaal PJ. Silent brain infarcts: a systematic review. Lancet Neurol 2007; 6: 611–619. - PubMed
-
- World Health Organization. ICD-11 for Mortality and Morbidity Statistics (Version: 02/2022). Published 2022. https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/126147...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
