

Uterine cervical stenosis: from classification to advances in management. Overcoming the obstacles to access the uterine cavity
- PMID: 37428263
- PMCID: PMC10866788
- DOI: 10.1007/s00404-023-07126-1
Uterine cervical stenosis: from classification to advances in management. Overcoming the obstacles to access the uterine cavity
Abstract
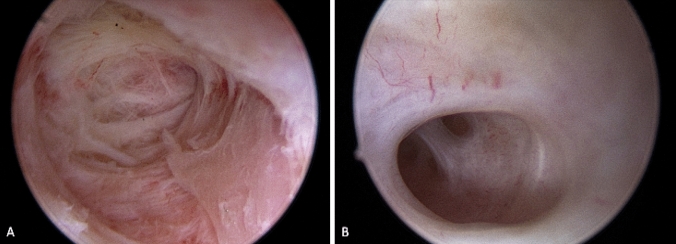
Background: To date hysteroscopy is the gold standard technique for the evaluation and management of intrauterine pathologies. The cervical canal represents the access route to the uterine cavity. The presence of cervical stenosis often makes entry into the uterine cavity difficult and occasionally impossible. Cervical stenosis has a multifactorial etiology. It is the result of adhesion processes that can lead to the narrowing or total obliteration of the cervical canal.
Purpose: In this review, we summarize the scientific evidence about cervical stenosis, aiming to identify the best strategy to overcome this challenging condition.
Methods: The literature review followed the scale for the quality assessment of narrative review articles (SANRA). All articles describing the hysteroscopic management of cervical stenosis were considered eligible. Only original papers that reported data on the topic were included.
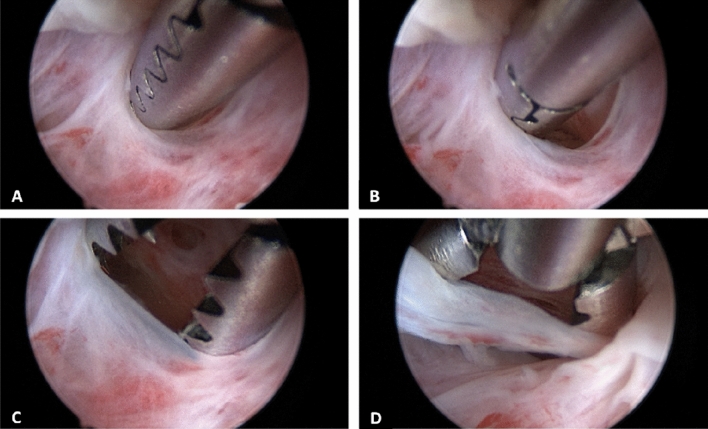
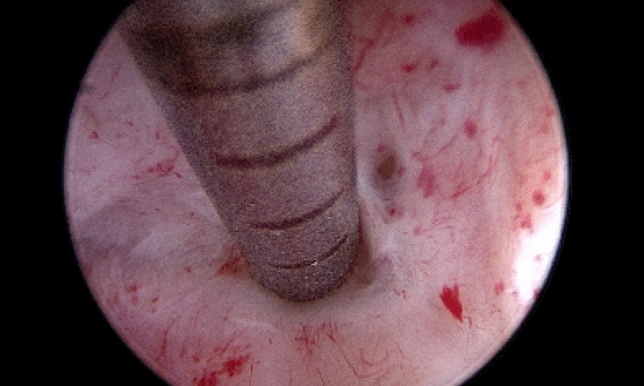
Results: Various strategies have been proposed to address cervical stenosis, including surgical and non-surgical methods. Medical treatments such as the preprocedural use of cervical-ripening agents or osmotic dilators have been explored. Surgical options include the use of cervical dilators and hysteroscopic treatments.
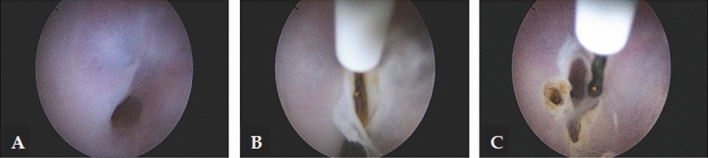
Conclusions: Cervical stenosis can present challenges in achieving successful intrauterine procedures. Operative hysteroscopy has been shown to have the highest success rate, particularly in cases of severe cervical stenosis, and is currently considered the gold standard for managing this condition. Despite the availability of miniaturized instruments that have made the management of cervical stenosis more feasible, it remains a complex task, even for experienced hysteroscopists.
Keywords: Cervical stenosis; Hysteroscopy; Infertility; Therapy.
© 2023. The Author(s).
Conflict of interest statement
The authors have no relevant financial or non-financial interests to disclose.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
