

Covid-19 triage in the emergency department 2.0: how analytics and AI transform a human-made algorithm for the prediction of clinical pathways
- PMID: 37428304
- PMCID: PMC10485125
- DOI: 10.1007/s10729-023-09647-2
Covid-19 triage in the emergency department 2.0: how analytics and AI transform a human-made algorithm for the prediction of clinical pathways
Abstract
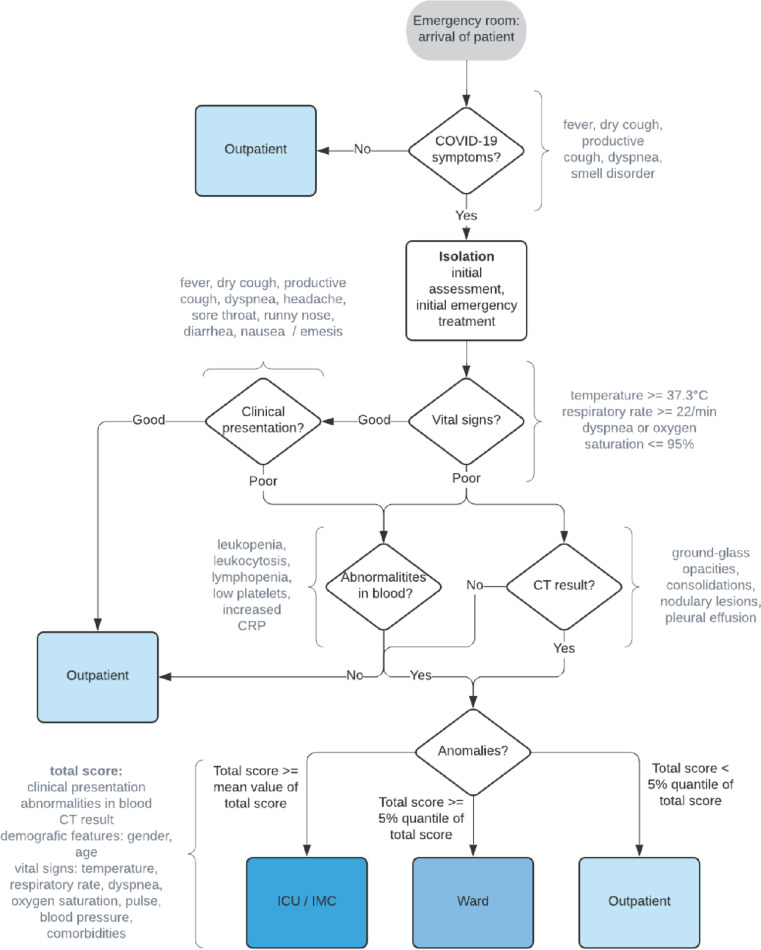
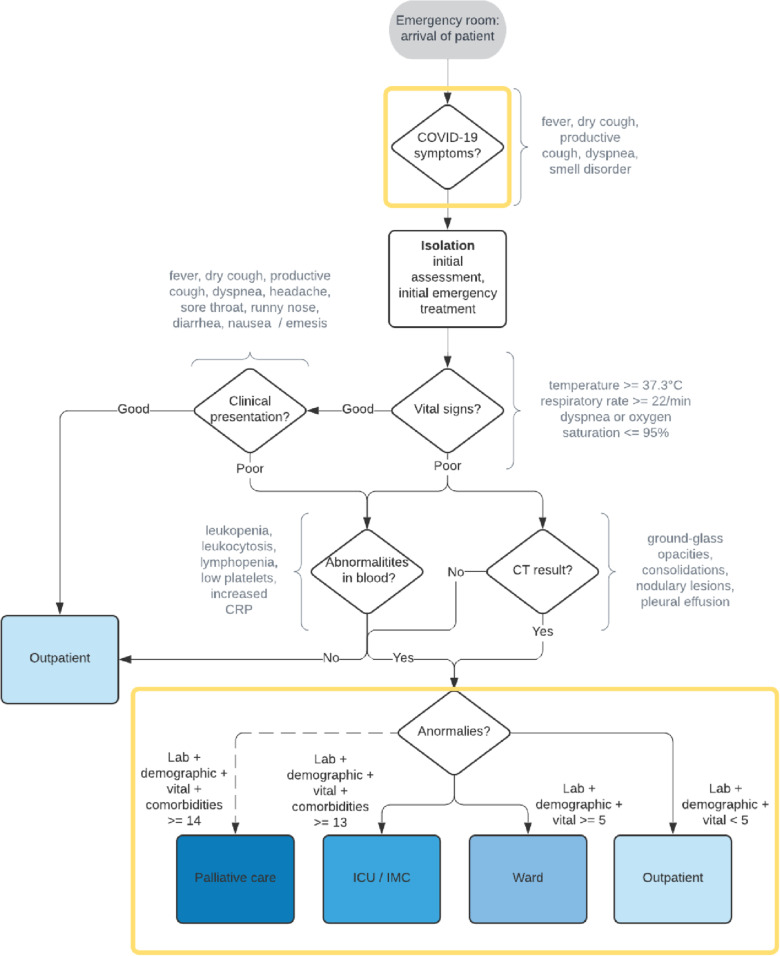
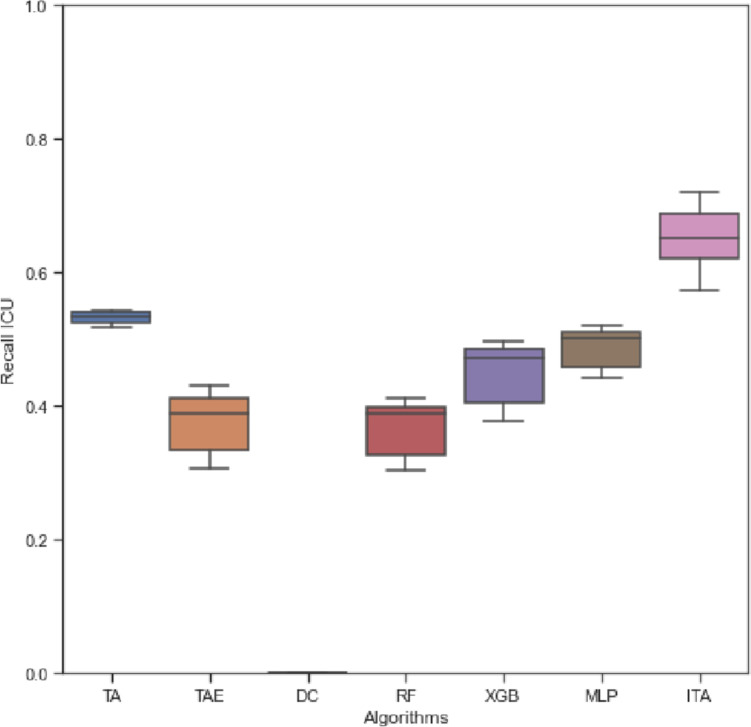
The Covid-19 pandemic has pushed many hospitals to their capacity limits. Therefore, a triage of patients has been discussed controversially primarily through an ethical perspective. The term triage contains many aspects such as urgency of treatment, severity of the disease and pre-existing conditions, access to critical care, or the classification of patients regarding subsequent clinical pathways starting from the emergency department. The determination of the pathways is important not only for patient care, but also for capacity planning in hospitals. We examine the performance of a human-made triage algorithm for clinical pathways which is considered a guideline for emergency departments in Germany based on a large multicenter dataset with over 4,000 European Covid-19 patients from the LEOSS registry. We find an accuracy of 28 percent and approximately 15 percent sensitivity for the ward class. The results serve as a benchmark for our extensions including an additional category of palliative care as a new label, analytics, AI, XAI, and interactive techniques. We find significant potential of analytics and AI in Covid-19 triage regarding accuracy, sensitivity, and other performance metrics whilst our interactive human-AI algorithm shows superior performance with approximately 73 percent accuracy and up to 76 percent sensitivity. The results are independent of the data preparation process regarding the imputation of missing values or grouping of comorbidities. In addition, we find that the consideration of an additional label palliative care does not improve the results.
Keywords: Artificial intelligence; Clinical decision making; Covid-19 triage; Machine learning; Predictive analytics.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Ardabili SF, Mosavi A, Ghamisi P, Ferdinand F, Varkonyi-Koczy AR, Reuter U, Rabczuk T, Atkinson PM. COVID-19 outbreak prediction with machine learning. Algorithms. 2020;13(10):1–36. doi: 10.3390/a13100249. - DOI
-
- Arrieta AB, Díaz-Rodríguez N, Del Ser J, Bennetot A, Tabik S, Barbado A, Garcia S, Gil-Lopez S, Molina D, Benjamins R, Chatila R, Herrera F. Explainable Artificial Intelligence (XAI): Concepts, taxonomies, opportunities and challenges toward responsible AI. Inf Fusion. 2020;58:82–115. doi: 10.1016/j.inffus.2019.12.012. - DOI
-
- Bartenschlager CC, Ebel SS, Kling S, Vehreschild J, Zabel LT, Spinner CD, Schuler A, Heller AR, Borgmann S, Hoffmann R, Rieg S, Messmann H, Hower M, Brunner JO, Hanses F, Römmele C (2022) COVIDAL: a machine learning classifier for digital COVID-19 diagnosis in German hospitals, Working paper, University of Augsburg
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
