

Abatacept, Cenicriviroc, or Infliximab for Treatment of Adults Hospitalized With COVID-19 Pneumonia: A Randomized Clinical Trial
- PMID: 37428480
- PMCID: PMC10334296
- DOI: 10.1001/jama.2023.11043
Abatacept, Cenicriviroc, or Infliximab for Treatment of Adults Hospitalized With COVID-19 Pneumonia: A Randomized Clinical Trial
Abstract
Importance: Immune dysregulation contributes to poorer outcomes in COVID-19.
Objective: To investigate whether abatacept, cenicriviroc, or infliximab provides benefit when added to standard care for COVID-19 pneumonia.
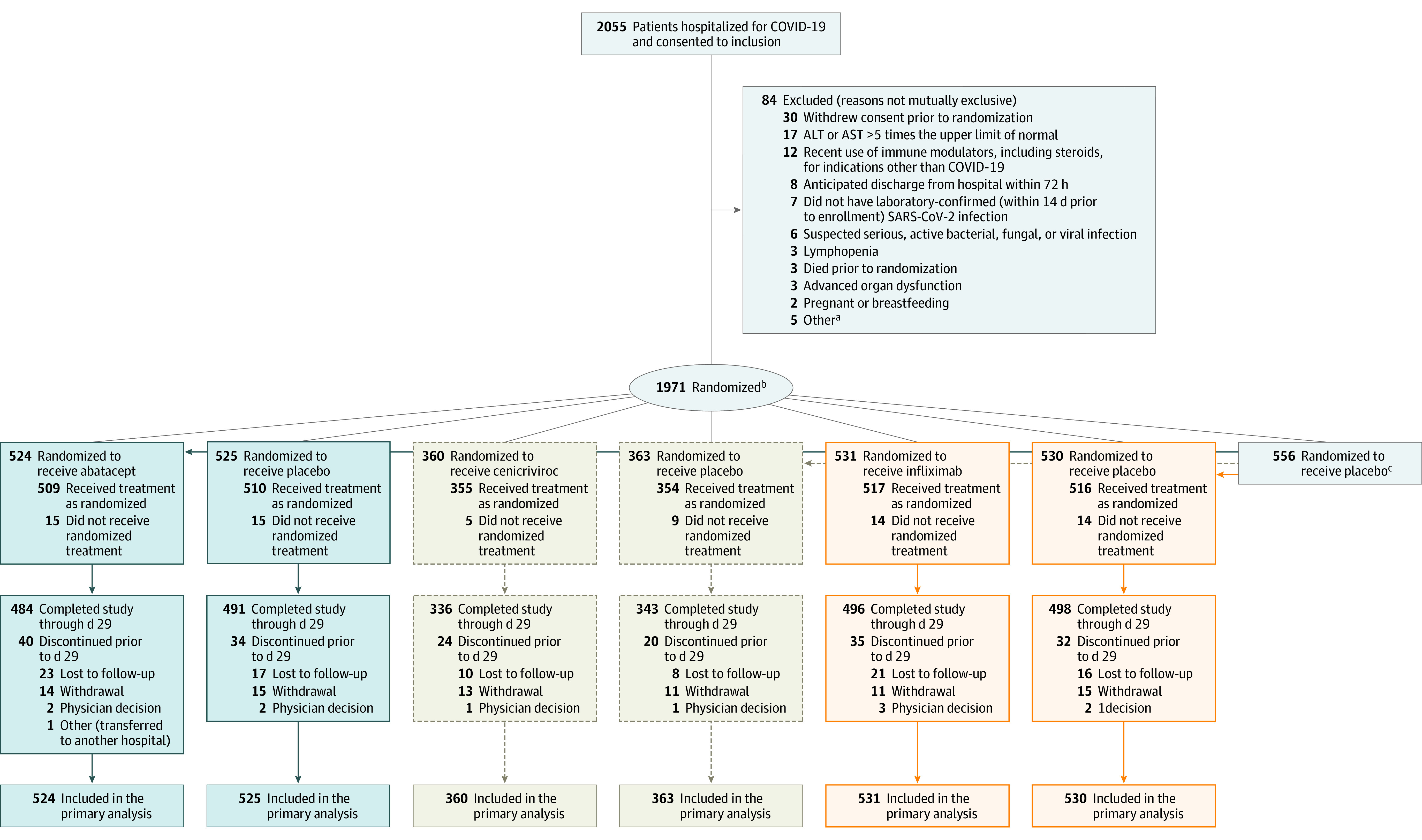
Design, setting, and participants: Randomized, double-masked, placebo-controlled clinical trial using a master protocol to investigate immunomodulators added to standard care for treatment of participants hospitalized with COVID-19 pneumonia. The results of 3 substudies are reported from 95 hospitals at 85 clinical research sites in the US and Latin America. Hospitalized patients 18 years or older with confirmed SARS-CoV-2 infection within 14 days and evidence of pulmonary involvement underwent randomization between October 2020 and December 2021.
Interventions: Single infusion of abatacept (10 mg/kg; maximum dose, 1000 mg) or infliximab (5 mg/kg) or a 28-day oral course of cenicriviroc (300-mg loading dose followed by 150 mg twice per day).
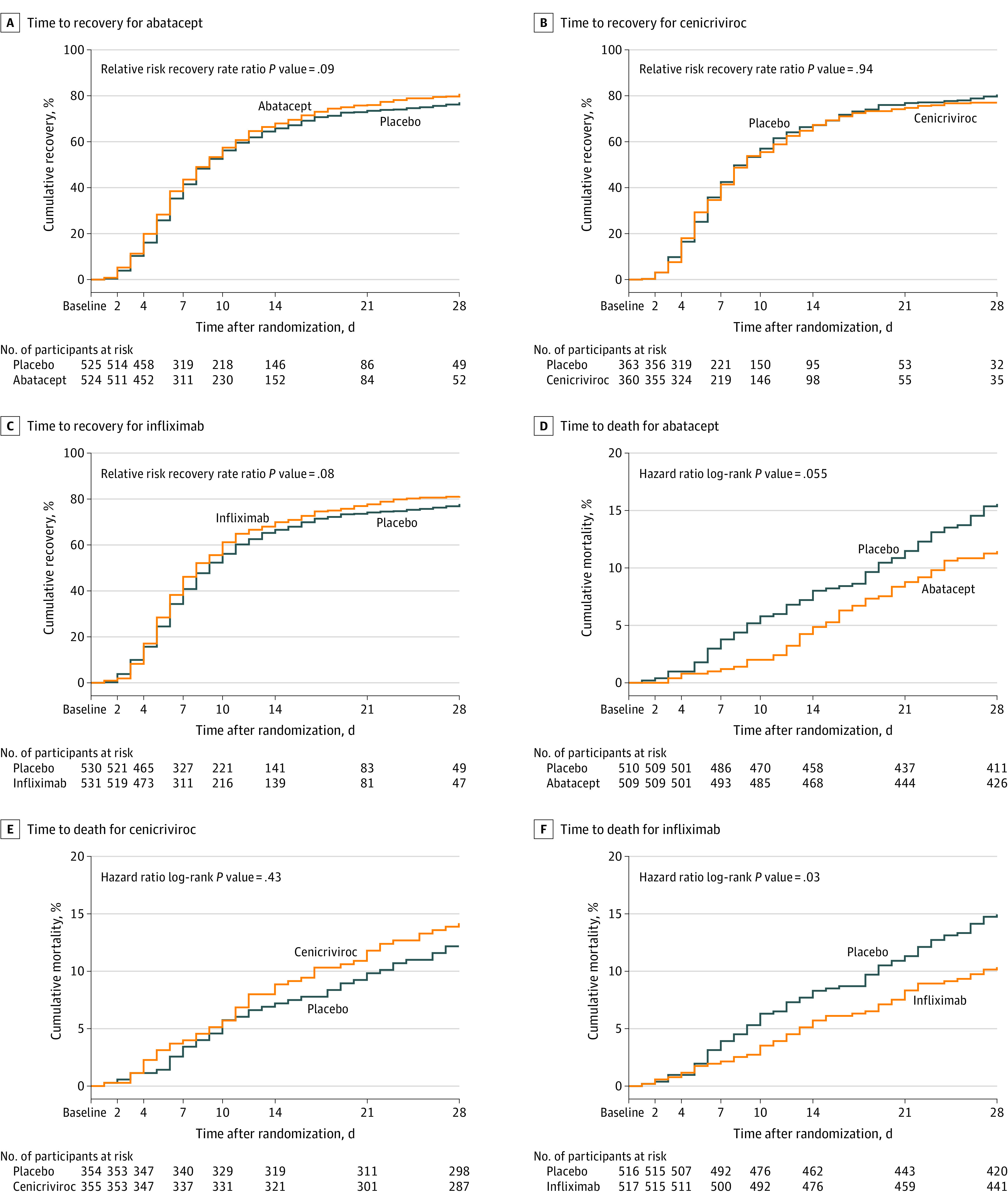
Main outcomes and measures: The primary outcome was time to recovery by day 28 evaluated using an 8-point ordinal scale (higher scores indicate better health). Recovery was defined as the first day the participant scored at least 6 on the ordinal scale.
Results: Of the 1971 participants randomized across the 3 substudies, the mean (SD) age was 54.8 (14.6) years and 1218 (61.8%) were men. The primary end point of time to recovery from COVID-19 pneumonia was not significantly different for abatacept (recovery rate ratio [RRR], 1.12 [95% CI, 0.98-1.28]; P = .09), cenicriviroc (RRR, 1.01 [95% CI, 0.86-1.18]; P = .94), or infliximab (RRR, 1.12 [95% CI, 0.99-1.28]; P = .08) compared with placebo. All-cause 28-day mortality was 11.0% for abatacept vs 15.1% for placebo (odds ratio [OR], 0.62 [95% CI, 0.41-0.94]), 13.8% for cenicriviroc vs 11.9% for placebo (OR, 1.18 [95% CI 0.72-1.94]), and 10.1% for infliximab vs 14.5% for placebo (OR, 0.59 [95% CI, 0.39-0.90]). Safety outcomes were comparable between active treatment and placebo, including secondary infections, in all 3 substudies.
Conclusions and relevance: Time to recovery from COVID-19 pneumonia among hospitalized participants was not significantly different for abatacept, cenicriviroc, or infliximab vs placebo.
Trial registration: ClinicalTrials.gov Identifier: NCT04593940.
Conflict of interest statement
Figures
Comment in
-
Translating Clinical Trial Results to Clinical Practice During a Pandemic.JAMA. 2023 Jul 25;330(4):321-322. doi: 10.1001/jama.2023.11260. JAMA. 2023. PMID: 37428492 No abstract available.
-
Treatment of Adults Hospitalized With COVID-19 Pneumonia.JAMA. 2023 Dec 5;330(21):2122-2123. doi: 10.1001/jama.2023.20406. JAMA. 2023. PMID: 38051331 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UL1 TR002544/TR/NCATS NIH HHS/United States
- UL1 TR001998/TR/NCATS NIH HHS/United States
- UL1 TR001881/TR/NCATS NIH HHS/United States
- UL1 TR003107/TR/NCATS NIH HHS/United States
- UL1 TR002645/TR/NCATS NIH HHS/United States
- UL1 TR001453/TR/NCATS NIH HHS/United States
- UL1 TR003017/TR/NCATS NIH HHS/United States
- UL1 TR002553/TR/NCATS NIH HHS/United States
- UL1 TR003096/TR/NCATS NIH HHS/United States
- UL1 TR002319/TR/NCATS NIH HHS/United States
- UL1 TR001445/TR/NCATS NIH HHS/United States
- UL1 TR002345/TR/NCATS NIH HHS/United States
- U24 TR001579/TR/NCATS NIH HHS/United States
- UL1 TR002366/TR/NCATS NIH HHS/United States
- UL1 TR002377/TR/NCATS NIH HHS/United States
- U24 TR001608/TR/NCATS NIH HHS/United States
- UL1 TR002489/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
