

Telemedicine-Based Management of Oral Anticoagulation Therapy: Systematic Review and Meta-analysis
- PMID: 37428532
- PMCID: PMC10366670
- DOI: 10.2196/45922
Telemedicine-Based Management of Oral Anticoagulation Therapy: Systematic Review and Meta-analysis
Abstract
Background: Oral anticoagulation is the cornerstone treatment of several diseases. Its management is often challenging, and different telemedicine strategies have been implemented to support it.
Objective: The aim of the study is to systematically review the evidence on the impact of telemedicine-based oral anticoagulation management compared to usual care on thromboembolic and bleeding events.
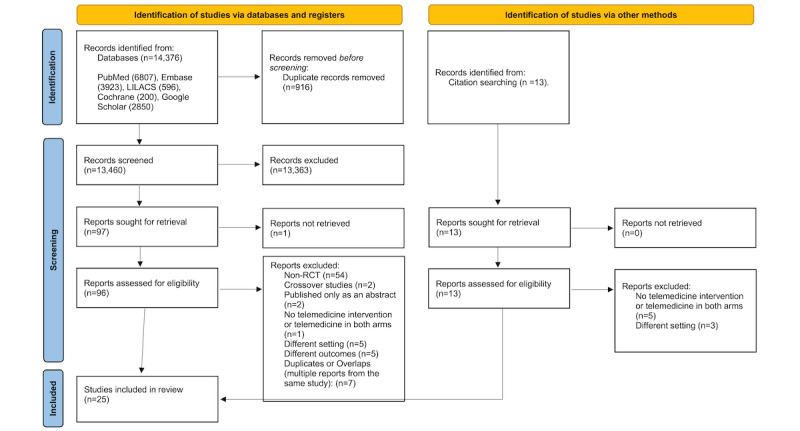
Methods: Randomized controlled trials were searched in 5 databases from inception to September 2021. Two independent reviewers performed study selection and data extraction. Total thromboembolic events, major bleeding, mortality, and time in therapeutic range were assessed. Results were pooled using random effect models.
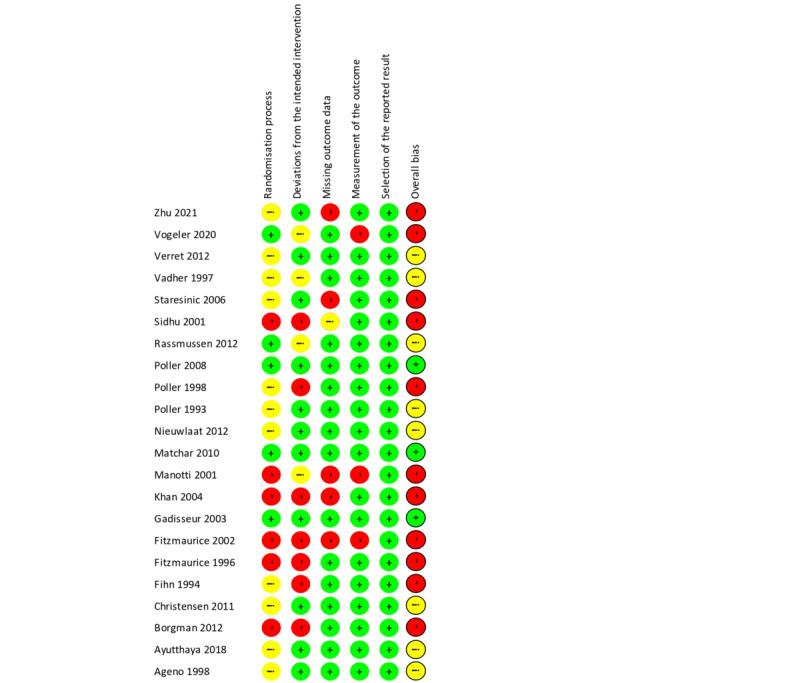
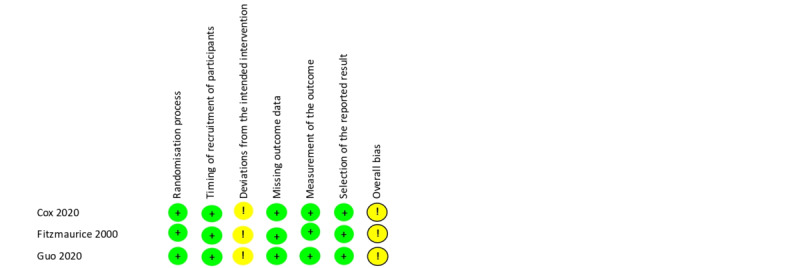
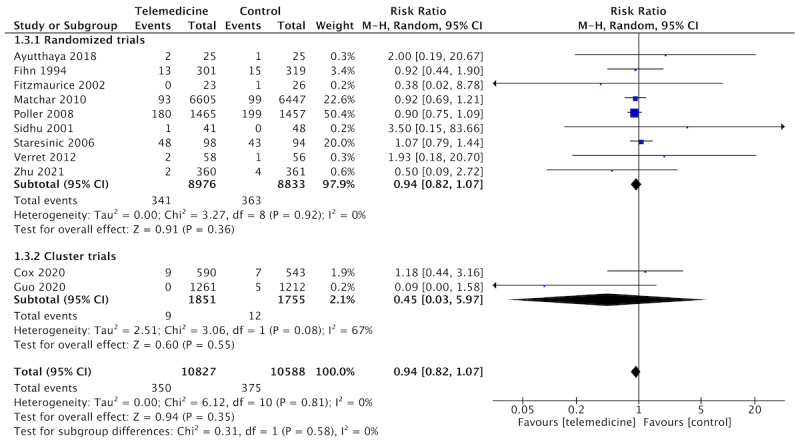
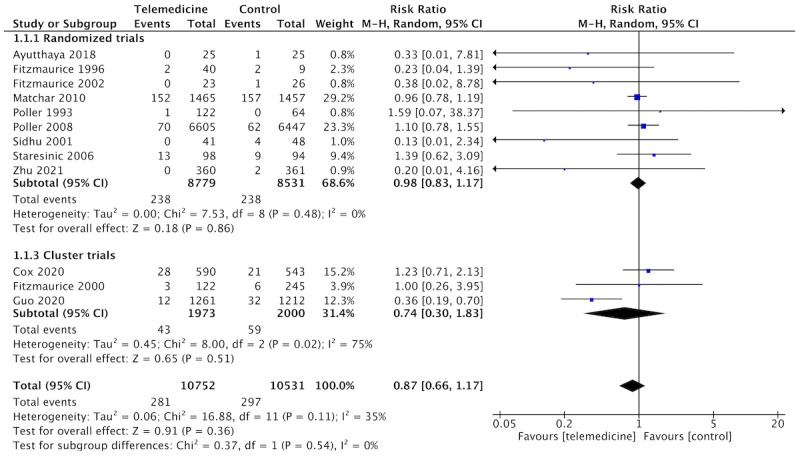
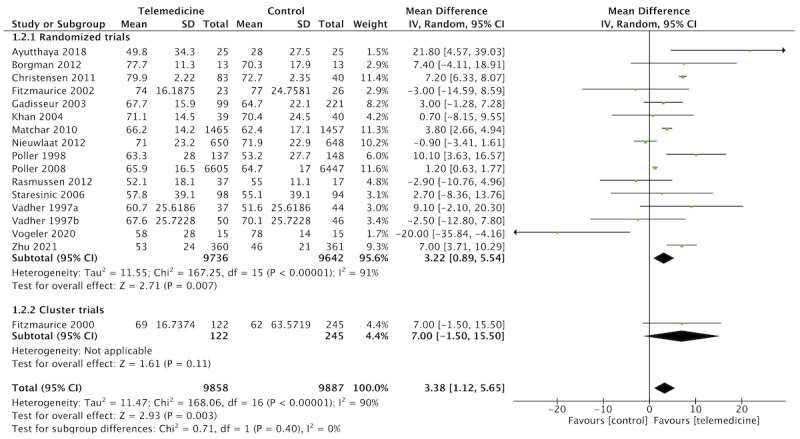
Results: In total, 25 randomized controlled trials were included (n=25,746 patients) and classified as moderate to high risk of bias by the Cochrane tool. Telemedicine resulted in lower rates of thromboembolic events, though not statistically significant (n=13 studies, relative risk [RR] 0.75, 95% CI 0.53-1.07; I2=42%), comparable rates of major bleeding (n=11 studies, RR 0.94, 95% CI 0.82-1.07; I2=0%) and mortality (n=12 studies, RR 0.96, 95% CI 0.78-1.20; I2=11%), and an improved time in therapeutic range (n=16 studies, mean difference 3.38, 95% CI 1.12-5.65; I2=90%). In the subgroup of the multitasking intervention, telemedicine resulted in an important reduction of thromboembolic events (RR 0.20, 95% CI 0.08-0.48).
Conclusions: Telemedicine-based oral anticoagulation management resulted in similar rates of major bleeding and mortality, a trend for fewer thromboembolic events, and better anticoagulation quality compared to standard care. Given the potential benefits of telemedicine-based care, such as greater access to remote populations or people with ambulatory restrictions, these findings may encourage further implementation of eHealth strategies for anticoagulation management, particularly as part of multifaceted interventions for integrated care of chronic diseases. Meanwhile, researchers should develop higher-quality evidence focusing on hard clinical outcomes, cost-effectiveness, and quality of life.
Trial registration: PROSPERO International Prospective Register of Systematic Reviews CRD42020159208; https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=159208.
Keywords: DOACs; anticoagulation; atrial fibrillation; eHealth; telemedicine; warfarin.
©Letícia Braga Ferreira, Rodrigo Lanna de Almeida, Alair Arantes, Hebatullah Abdulazeem, Ishanka Weerasekara, Leticia Santos Dias Norberto Ferreira, Luana Fonseca de Almeida Messias, Luciana Siuves Ferreira Couto, Maria Auxiliadora Parreiras Martins, Núbia Suelen Antunes, Raissa Carolina Fonseca Cândido, Samuel Rosa Ferreira, Tati Guerra Pezzini Assis, Thais Marques Pedroso, Eric Boersma, Antonio Ribeiro, Milena Soriano Marcolino. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 10.07.2023.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures

References
-
- Kornej J, Börschel CS, Benjamin EJ, Schnabel RB. Epidemiology of atrial fibrillation in the 21st century: novel methods and new insights. Circ Res. 2020;127(1):4–20. doi: 10.1161/CIRCRESAHA.120.316340. https://europepmc.org/abstract/MED/32716709 - DOI - PMC - PubMed
-
- Yu AYX, Malo S, Svenson LW, Wilton SB, Hill MD. Temporal trends in the use and comparative effectiveness of direct oral anticoagulant agents versus warfarin for nonvalvular atrial fibrillation: a Canadian population-based study. J Am Heart Assoc. 2017;6(11):e007129. doi: 10.1161/JAHA.117.007129. https://www.ahajournals.org/doi/10.1161/JAHA.117.007129?url_ver=Z39.88-2... JAHA.117.007129 - DOI - PMC - PubMed
-
- Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, Capodanno D, Conradi L, De Bonis M, De Paulis R, Delgado V, Freemantle N, Gilard M, Haugaa KH, Jeppsson A, Jüni P, Pierard L, Prendergast BD, Sádaba JR, Tribouilloy C, Wojakowski W, ESC/EACTS Scientific Document Group 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J. 2022;43(7):561–632. doi: 10.1093/eurheartj/ehab395. https://hdl.handle.net/2268/291297 6358470 - DOI - PubMed
-
- Connolly SJ, Karthikeyan G, Ntsekhe M, Haileamlak A, El Sayed A, El Ghamrawy A, Damasceno A, Avezum A, Dans AML, Gitura B, Hu D, Kamanzi ER, Maklady F, Fana G, Gonzalez-Hermosillo JA, Musuku J, Kazmi K, Zühlke L, Gondwe L, Ma C, Paniagua M, Ogah OS, Molefe-Baikai OJ, Lwabi P, Chillo P, Sharma SK, Cabral TTJ, Tarhuni WM, Benz A, van Eikels M, Krol A, Pattath D, Balasubramanian K, Rangarajan S, Ramasundarahettige C, Mayosi B, Yusuf S, INVICTUS Investigators Rivaroxaban in rheumatic heart disease-associated atrial fibrillation. N Engl J Med. 2022;387(11):978–988. doi: 10.1056/NEJMoa2209051. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
