

Incidence and Risk Factors for Hepatocellular Carcinoma in Cirrhosis: The Multicenter Hepatocellular Carcinoma Early Detection Strategy (HEDS) Study
- PMID: 37429366
- PMCID: PMC10529044
- DOI: 10.1053/j.gastro.2023.06.027
Incidence and Risk Factors for Hepatocellular Carcinoma in Cirrhosis: The Multicenter Hepatocellular Carcinoma Early Detection Strategy (HEDS) Study
Abstract
Background & aims: Worldwide, hepatocellular carcinoma (HCC) is a common malignancy. We aimed to prospectively determine the incidence and risk factors of HCC in a U.S.
Methods: The multicenter Hepatocellular Carcinoma Early Detection Strategy study of the National Institutes of Health prospectively enrolled patients with cirrhosis who underwent standard surveillance for HCC. Demographics, medical and family history, etiology of liver disease, and clinical features were evaluated for associations with HCC.
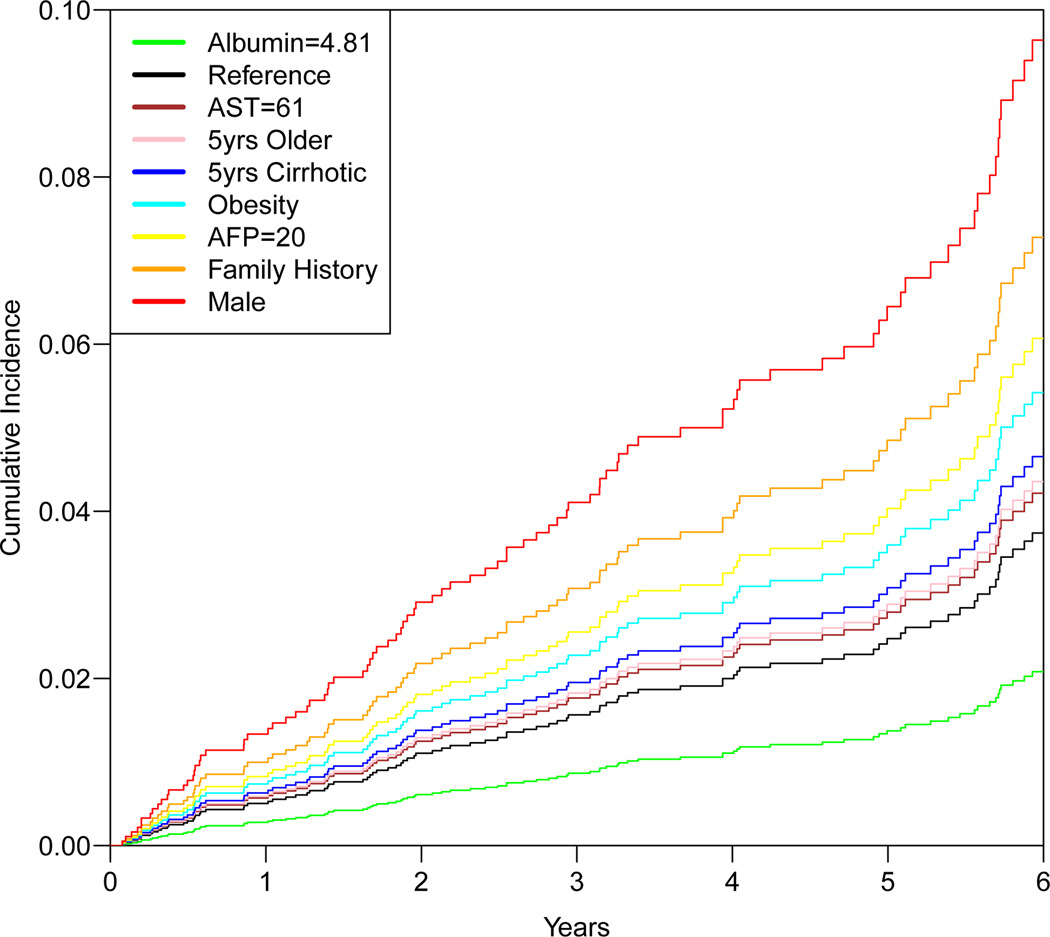
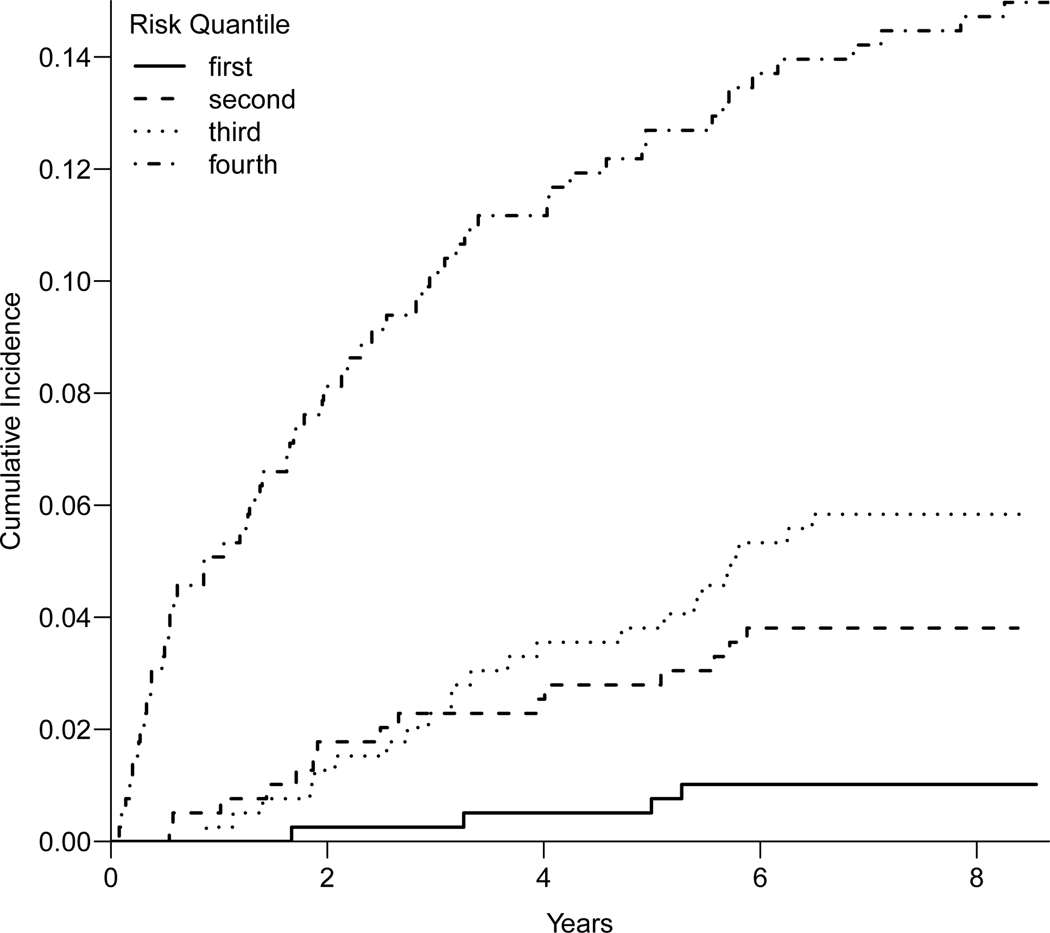
Results: Between April 10, 2013 and December 31, 2021, 1723 patients were enrolled and confirmed eligible. During median follow-up of 2.2 years (range, 0-8.7 years), there were 109 incident cases of HCC for an incidence rate of 2.4 per 100 person-years: 88 (81%) patients with very early/early Barcelona Clinic Liver Cancer stage (0, A), 20 (18%) intermediate stage (B), and 1 (1%) unknown stage. Risk factor analyses were restricted to 1325 patients, including 95 incident HCC, with at least 6 months of follow-up. The majority were men (53.2%), obese or severely obese (median body mass index, 30.2 kg/m2), and white (86.3%); 42.0% had history of hepatitis C virus infection, 20.7% had alcoholic liver disease, and 24.9% had nonalcoholic fatty liver disease. Fourteen risk factors for HCC were significant (P < .05) in univariate analyses, and a multivariate subset was selected using stepwise logistic regression. The multivariate subset contained gender (P < .001; male; odds ratio [OR], 2.47; 95% confidence interval [CI], 1.54-4.07), years with cirrhosis (P = .004; OR, 1.06; 95% CI, 1.02-1.1), family history of liver cancer (P = .02; yes; OR, 2.69; 95% CI, 1.11-5.86), age (per 5 years; P = .02; OR, 1.17; 95% CI, 1.03-1.33), obesity (P = .02; yes; OR, 1.7; 95% CI, 1.08-2.73), aspartate aminotransferase (log(1+AST); P = .06; OR, 1.54; 95% CI, 0.97-2.42), alpha-fetoprotein (log(1+AFP); P = .07; OR, 1.32; 95% CI, 0.97-1.77), and albumin (P = .10; OR, 0.7; 95% CI, 0.46-1.07).
Conclusions: Thus far, this is the largest prospective and geographically diverse study of a U.S. cohort of patients with cirrhosis that validates known risk factors for HCC (gender, age, obesity, years with cirrhosis, family history of liver cancer, baseline AFP, albumin, and AST). The incidence of HCC was 2.4% per 100 person-years.
Keywords: Cirrhosis; Early Detection Research Network; Hepatocellular Carcinoma; Risk Factors.
Copyright © 2023 AGA Institute. All rights reserved.
Figures
References
-
- Davila JA, Morgan RO, Shaib Y, McGlynn KA, El-Serag HB. Hepatitis C infection and the increasing incidence of hepatocellular carcinoma: a population-based study. Gastroenterology 2004;127:1372–1380. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
