

Atypical functional connectivity hierarchy in Rolandic epilepsy
- PMID: 37429897
- PMCID: PMC10333191
- DOI: 10.1038/s42003-023-05075-8
Atypical functional connectivity hierarchy in Rolandic epilepsy
Abstract
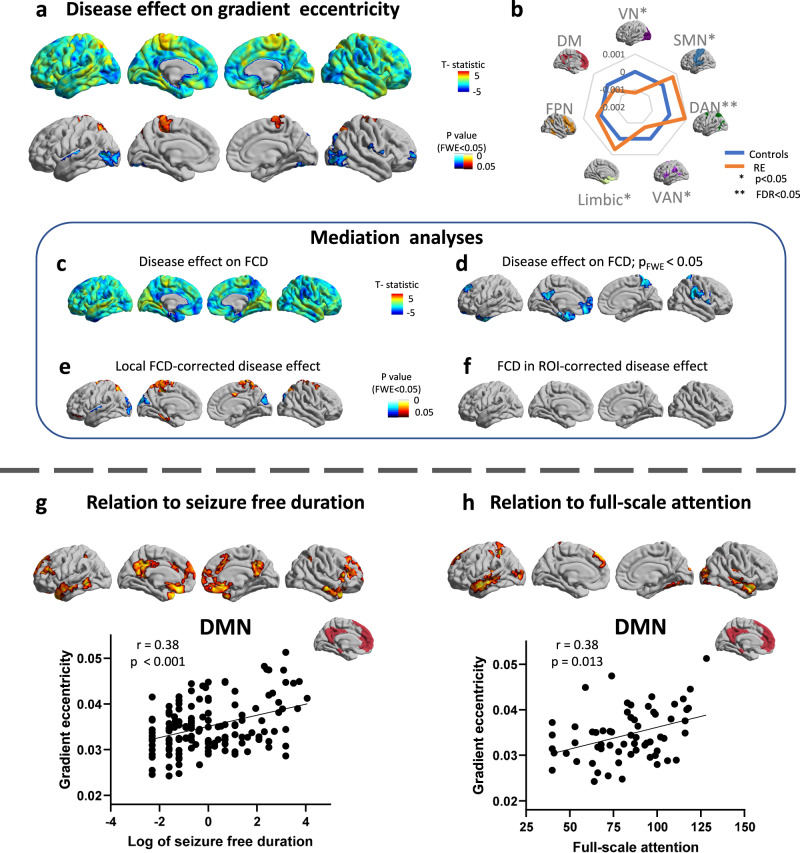
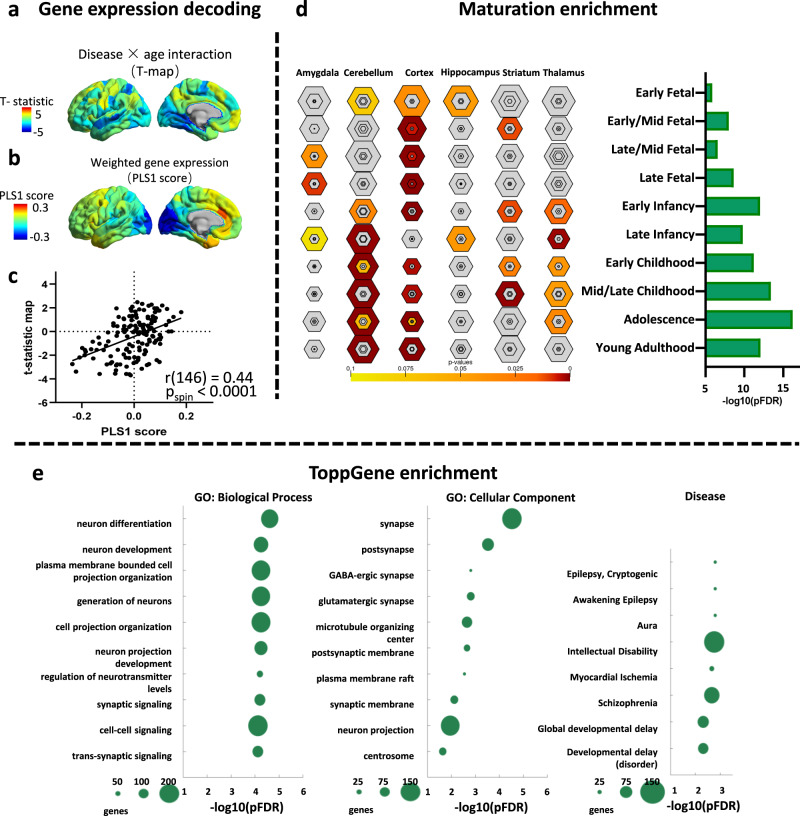
Functional connectivity hierarchy is an important principle in the process of brain functional organization and an important feature reflecting brain development. However, atypical brain network hierarchy organization in Rolandic epilepsy have not been systematically investigated. We examined connectivity alteration with age and its relation to epileptic incidence, cognition, or underlying genetic factors in 162 cases of Rolandic epilepsy and 117 typically developing children, by measuring fMRI multi-axis functional connectivity gradients. Rolandic epilepsy is characterized by contracting and slowing expansion of the functional connectivity gradients, highlighting the atypical age-related change of the connectivity hierarchy in segregation properties. The gradient alterations are relevant to seizure incidence, cognition, and connectivity deficit, and development-associated genetic basis. Collectively, our approach provides converging evidence for atypical connectivity hierarchy as a system-level substrate of Rolandic epilepsy, suggesting this is a disorder of information processing across multiple functional domains, and established a framework for large-scale brain hierarchical research.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
