

Short-term effects of an elimination diet and healthy diet in children with attention-deficit/hyperactivity disorder: a randomized-controlled trial
- PMID: 37430148
- PMCID: PMC11098970
- DOI: 10.1007/s00787-023-02256-y
Short-term effects of an elimination diet and healthy diet in children with attention-deficit/hyperactivity disorder: a randomized-controlled trial
Abstract
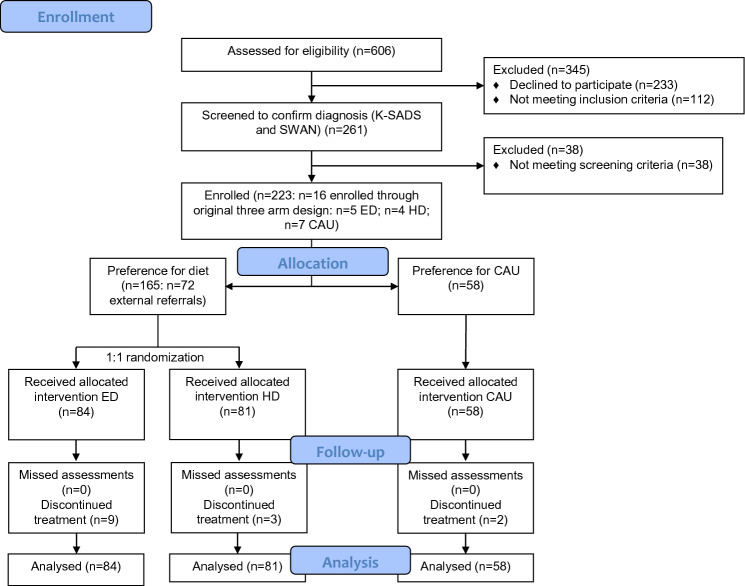
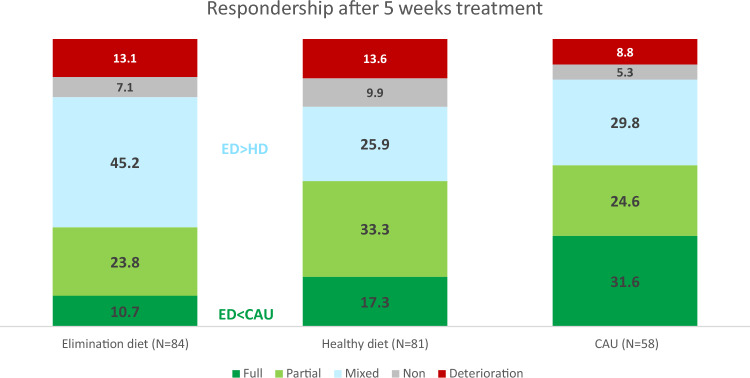
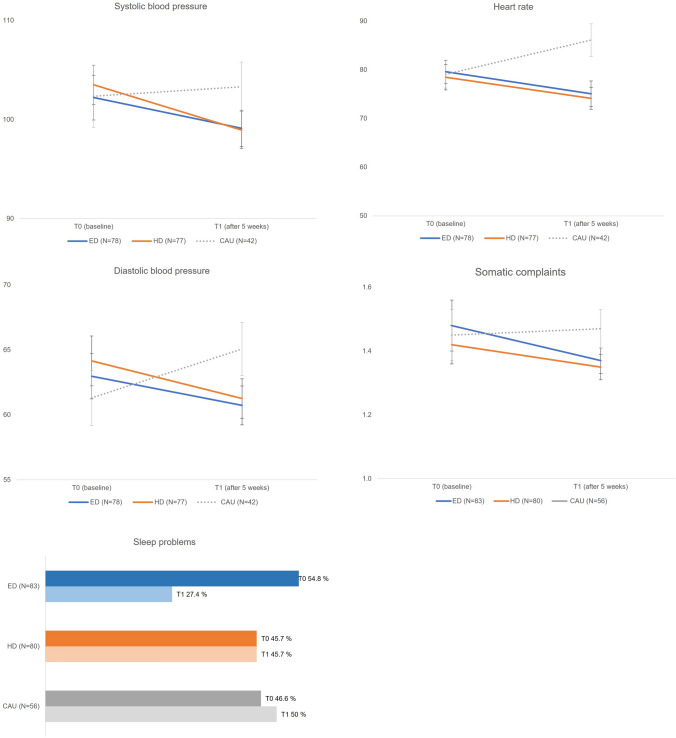
An Elimination Diet (ED) may be effective in reducing symptoms of Attention-Deficit/Hyperactivity Disorder (ADHD), but has never been compared to an active control condition [i.e., Healthy Diet (HD)]. In a two-armed RCT, a total of N = 165 children (5-12 years) with ADHD were randomized by means of minimization (1:1) to either an ED (N = 84) or HD (N = 81) within two Dutch child and adolescent psychiatry centers. The design included a non-randomized comparator arm including N = 58 children being treated with Care as Usual (CAU). Treatment allocation was unblinded. The primary outcome was a 5-point ordinal measure of respondership based on a combination of parent and teacher ratings on ADHD and emotion regulation, determined after 5 weeks of treatment. Ordinal regression analyses were done on an intention-to-treat basis. Fewer ED (35%) than HD (51%) participants showed a partial to full response, despite overall good-to-excellent treatment adherence (> 88%) and comparable high parental prior believes. A younger age and higher problem severity predicted a better respondership. CAU-preferring participants responded more often favorably (56%) compared to ED-but not HD-participants. Small-to-medium improvements in physical health (blood pressure, heart rate, and somatic complaints) were found in response to ED/HD versus decrements in response to CAU (74% received psychostimulants). The lack of superiority of the ED versus HD suggests that for the majority of children, dietary treatment response is not rooted in food-allergies/-sensitivities. The comparable results for treatment with HD and CAU are remarkable given that CAU participants were probably 'easier to treat' than HD (and ED) participants with proportionally fewer with a (suboptimal/non-response to) prior treatment with medication (4% versus 20%). Further assessment of long-term effects is needed to evaluate the potential place of dietary treatment within clinical guidelines. The trial is closed and registered in the Dutch trial registry, number NL5324 ( https://www.onderzoekmetmensen.nl/en/trial/25997 ).
Keywords: ADHD; Child psychiatry; Dietary treatment; Emotion regulation.
© 2023. The Author(s).
Conflict of interest statement
JB reports delivering consults to a drug company, for which he received fees outside the submitted work. JB and GvdL received personal fees and fees for the institution for presenting (outside the submitted work) at drug companies, a consultancy bureau, Radboud University, a dentist magazine and medical education. JB is a member of the Advisory Board for Medice, Angelini, and Servier. JD, RD, and HK are members of the Data Safety Monitoring Board of the TRACE study. All other authors declare that they have no competing interests.
Figures
References
-
- Schneider WF. Psychiatric evaluation of the hyperkinetic child. J Pediatr. 1945;26:559–570. doi: 10.1016/S0022-3476(45)80083-5. - DOI
-
- Pelsser LM, Frankena K, Toorman J, Pereira RR. Diet and ADHD, reviewing the evidence: A systematic review of meta-analyses of double-blind placebo-controlled trials evaluating the efficacy of diet interventions on the behavior of children with ADHD. PLoS One. 2017;12(1):e0169277. doi: 10.1371/journal.pone.0169277. - DOI - PMC - PubMed
-
- Nigg JT, Lewis K, Edinger T, Falk M. Meta-analysis of attention-deficit/hyperactivity disorder or attention-deficit/hyperactivity disorder symptoms, restriction diet, and synthetic food color additives. J Am Acad Child Adolesc Psychiatr. 2012;51(1):86–97. doi: 10.1016/j.jaac.2011.10.015. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- Eat2beNICE/Horizon 2020 Framework Programme
- Eat2beNICE/Horizon 2020 Framework Programme
- Eat2beNICE/Horizon 2020 Framework Programme
- Eat2beNICE/Horizon 2020 Framework Programme
- Eat2beNICE/Horizon 2020 Framework Programme
- Eat2beNICE/Horizon 2020 Framework Programme
- Eat2beNICE/Horizon 2020 Framework Programme
- Eat2beNICE/Horizon 2020 Framework Programme
- Eat2beNICE/Horizon 2020 Framework Programme
- Eat2beNICE/Horizon 2020 Framework Programme
- Eat2beNICE/Horizon 2020 Framework Programme
- Eat2beNICE/Horizon 2020 Framework Programme
- Eat2beNICE/Horizon 2020 Framework Programme
- Eat2beNICE/Horizon 2020 Framework Programme
- Eat2beNICE/Horizon 2020 Framework Programme
- Eat2beNICE/Horizon 2020 Framework Programme
- Eat2beNICE/Horizon 2020 Framework Programme
- 837002506/ZONMW_/ZonMw/Netherlands
- 837002506/ZONMW_/ZonMw/Netherlands
- 837002506/ZONMW_/ZonMw/Netherlands
- 837002506/ZONMW_/ZonMw/Netherlands
- 837002506/ZONMW_/ZonMw/Netherlands
- 837002506/ZONMW_/ZonMw/Netherlands
- 837002506/ZONMW_/ZonMw/Netherlands
- 837002506/ZONMW_/ZonMw/Netherlands
- 837002506/ZONMW_/ZonMw/Netherlands
- 837002506/ZONMW_/ZonMw/Netherlands
- 837002506/ZONMW_/ZonMw/Netherlands
- 837002506/ZONMW_/ZonMw/Netherlands
- 837002506/ZONMW_/ZonMw/Netherlands
- 837002506/ZONMW_/ZonMw/Netherlands
- 837002506/ZONMW_/ZonMw/Netherlands
LinkOut - more resources
Full Text Sources
Medical
Research Materials
