

The effect of intraoperative goal-directed fluid therapy combined with enhanced recovery after surgery program on postoperative complications in elderly patients undergoing thoracoscopic pulmonary resection: a prospective randomized controlled study
- PMID: 37430359
- PMCID: PMC10332062
- DOI: 10.1186/s13741-023-00327-x
The effect of intraoperative goal-directed fluid therapy combined with enhanced recovery after surgery program on postoperative complications in elderly patients undergoing thoracoscopic pulmonary resection: a prospective randomized controlled study
Abstract
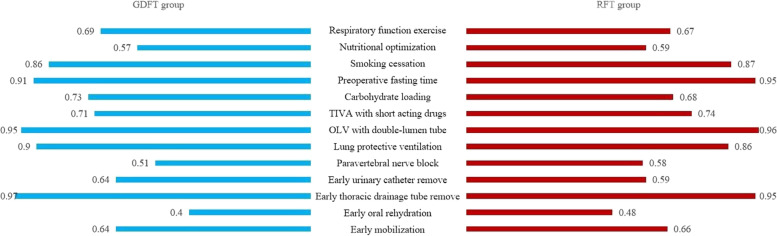
Background: To investigate the effect of intraoperative goal-directed fluid therapy (GDFT) combined with enhanced recovery after surgery (ERAS) program on postoperative complications in elderly patients undergoing thoracoscopic pulmonary resection.
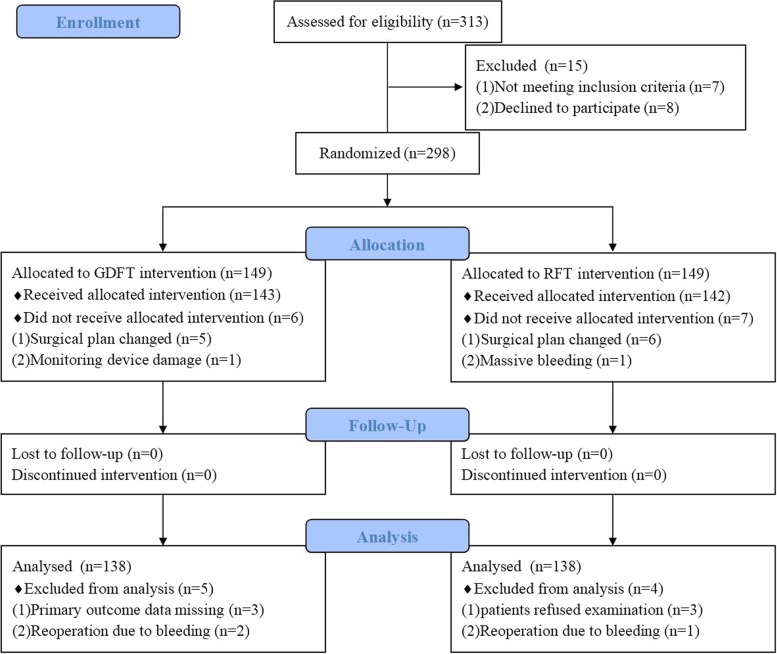
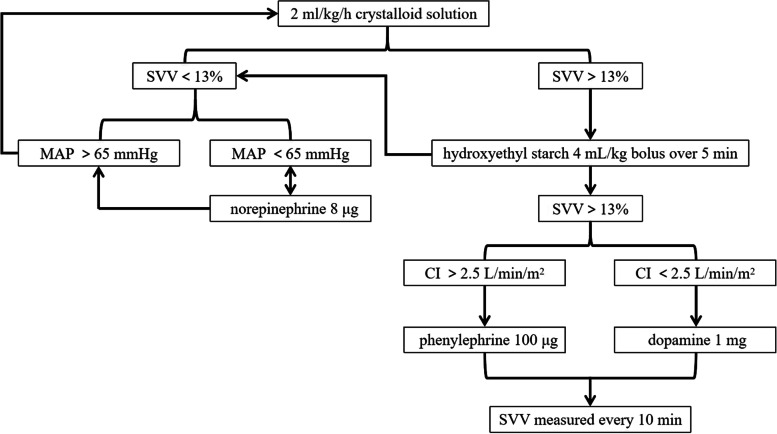
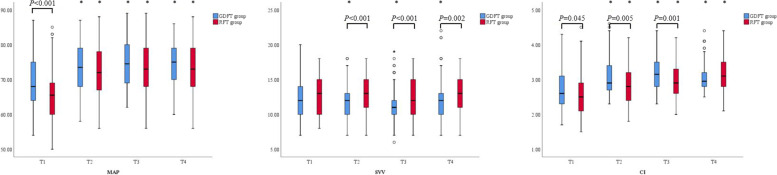
Methods: Patients, more than 60 years old, undergoing thoracoscopic pulmonary resection for non-small cell lung cancer were randomly divided into GDFT group and restrictive fluid therapy (RFT) group. ERAS program was implemented in all patients. In GDFT group, the intraoperative fluid management was guided by stroke volume variation (SVV), cardiac index (CI), and mean arterial pressure (MAP) and maintained the SVV < 13%, CI > 2.5 L/min/m2, and MAP > 65 mmHg. In RFT group, fluid maintenance with 2 ml/kg/h of balanced crystalloid solution, norepinephrine was used to maintain MAP > 65 mmHg. The incidence of postoperative acute kidney injury (AKI) and pulmonary and cardiac complications was compared.
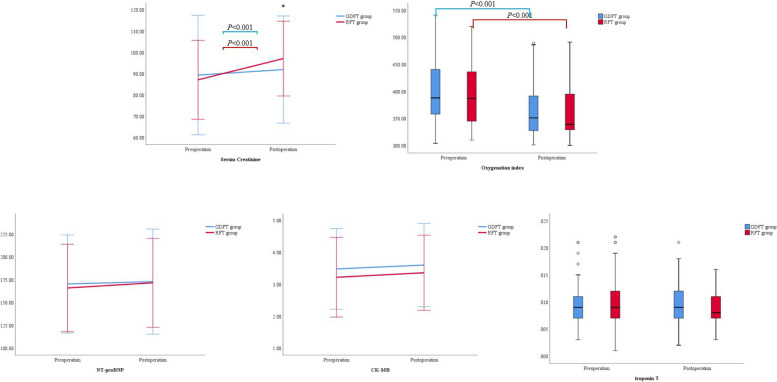
Results: Two-hundred seventy-six patients were enrolled and randomly divided into two groups (138 in each group). Compared to RFT group, the total intraoperative infusion volume, colloids infusion volume, and urine output were more; the dosage of norepinephrine was lower in GDFT group. Although there were no significant differences of postoperative AKI (GDFT vs RFT; 4.3% vs 8%; P = 0.317) and composite postoperative complications (GDFT vs RFT; 66 vs 70) between groups, but the postoperative increase degree of serum creatinine was lower in GDFT group than that in RFT group (GDFT vs RFT; 91.9 ± 25.2 μmol/L vs 97.1 ± 17.6 μmol/L; P = 0.048).
Conclusions: Under ERAS program, there was no significant difference of AKI incidence between GDFT and RFT in elderly patients undergoing thoracoscopic pulmonary resection. But postoperative increase degree of serum creatinine was lower in GDFT group.
Trial registration: Registered at ClinicalTrials.gov, NCT04302467 on 26 February 2020.
Keywords: Acute kidney injury; Enhanced recovery after surgery; Goal-directed fluid therapy; Pulmonary resection.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Effects of intraoperative goal-directed fluid therapy and restrictive fluid therapy combined with enhanced recovery after surgery protocol on complications after thoracoscopic lobectomy in high-risk patients: study protocol for a prospective randomized controlled trial.Trials. 2021 Jan 7;22(1):36. doi: 10.1186/s13063-020-04983-y. Trials. 2021. PMID: 33413593 Free PMC article.
-
Effect of low-dose norepinephrine combined with goal-directed fluid therapy on postoperative pulmonary complications in lung surgery: A prospective randomized controlled trial.J Clin Anesth. 2024 Dec;99:111645. doi: 10.1016/j.jclinane.2024.111645. Epub 2024 Oct 9. J Clin Anesth. 2024. PMID: 39388832 Clinical Trial.
-
Prospective comparison of the effects of intraoperative goal-directed fluid therapy and restrictive fluid therapy on complications in thoracoscopic lobectomy.J Int Med Res. 2021 Dec;49(12):3000605211062787. doi: 10.1177/03000605211062787. J Int Med Res. 2021. PMID: 34918965 Free PMC article. Clinical Trial.
-
Goal-directed fluid therapy does not reduce postoperative ileus in gastrointestinal surgery: A meta-analysis of randomized controlled trials.Medicine (Baltimore). 2018 Nov;97(45):e13097. doi: 10.1097/MD.0000000000013097. Medicine (Baltimore). 2018. PMID: 30407319 Free PMC article. Review.
-
Goal-directed fluid therapy versus conventional fluid therapy in colorectal surgery: A meta analysis of randomized controlled trials.Int J Surg. 2018 Aug;56:264-273. doi: 10.1016/j.ijsu.2018.06.034. Epub 2018 Jul 1. Int J Surg. 2018. PMID: 29972762 Review.
Cited by
-
Effects of fluid therapy combined with a preoperative glucose load regimen on postoperative recovery in patients with rectal cancer.World J Gastrointest Surg. 2024 Aug 27;16(8):2662-2670. doi: 10.4240/wjgs.v16.i8.2662. World J Gastrointest Surg. 2024. PMID: 39220080 Free PMC article.
-
No increase in chronic kidney disease after postoperative acute kidney injury in gynecologic oncologic ERAS surgery.Gynecol Oncol. 2025 Jul;198:168-175. doi: 10.1016/j.ygyno.2025.06.002. Epub 2025 Jun 11. Gynecol Oncol. 2025. PMID: 40505183
-
Permissive hypercapnia combined with goal-directed fluid therapy improve postoperative mental health in elderly patients undergoing laparoscopic surgery.World J Psychiatry. 2025 Jul 19;15(7):106023. doi: 10.5498/wjp.v15.i7.106023. eCollection 2025 Jul 19. World J Psychiatry. 2025. PMID: 40740450 Free PMC article.
References
-
- Arslantas MK, Kara HV, Tuncer BB, Yildizeli B, Yuksel M, Bostanci K, et al. Effect of the amount of intraoperative fluid administration on postoperative pulmonary complications following anatomic lung resections. J Thorac Cardiovasc Surg. 2015;149:314–20. doi: 10.1016/j.jtcvs.2014.08.071. - DOI - PubMed
-
- Batchelor TJP, Rasburn NJ, Berchtold EA, Brunelli A, Cerfolio RJ, Gonzalez M, et al. Guidelines for enhanced recovery after lung surgery: recommendations of the enhanced recovery after surgery (ERAS®) Society and the European Society of Thoracic Surgeons (ESTS) Eur J Cardiothorac Surg. 2019;55:91–115. doi: 10.1093/ejcts/ezy301. - DOI - PubMed
Associated data
Grants and funding
- XJTU1AF-CRF-2019-012/Grant support Clinical research project of the First Affiliated Hospital of Xi'an Jiaotong University
- XJTU1AF-CRF-2019-012/Grant support Clinical research project of the First Affiliated Hospital of Xi'an Jiaotong University
- XJTU1AF-CRF-2019-012/Grant support Clinical research project of the First Affiliated Hospital of Xi'an Jiaotong University
- XJTU1AF-CRF-2019-012/Grant support Clinical research project of the First Affiliated Hospital of Xi'an Jiaotong University
- XJTU1AF-CRF-2019-012/Grant support Clinical research project of the First Affiliated Hospital of Xi'an Jiaotong University
- XJTU1AF-CRF-2019-012/Grant support Clinical research project of the First Affiliated Hospital of Xi'an Jiaotong University
- XJTU1AF-CRF-2019-012/Grant support Clinical research project of the First Affiliated Hospital of Xi'an Jiaotong University
- XJTU1AF-CRF-2019-012/Grant support Clinical research project of the First Affiliated Hospital of Xi'an Jiaotong University
LinkOut - more resources
Full Text Sources
Medical
Research Materials
