

Anesthesia care provider sedation versus conscious sedation for endoscopic ultrasound-guided tissue acquisition: a retrospective cohort study
- PMID: 37430404
- PMCID: PMC10565438
- DOI: 10.5946/ce.2023.006
Anesthesia care provider sedation versus conscious sedation for endoscopic ultrasound-guided tissue acquisition: a retrospective cohort study
Abstract
Background/aims: We aimed to study the effects of sedation on endoscopic ultrasound-guided tissue acquisition.
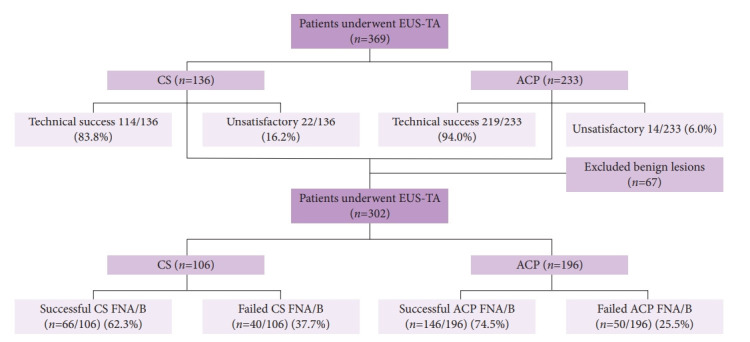
Methods: We conducted a retrospective study evaluating the role of sedation in endoscopic ultrasound-guided tissue acquisition by comparing two groups: anesthesia care provider (ACP) sedation and endoscopist-directed conscious sedation (CS).
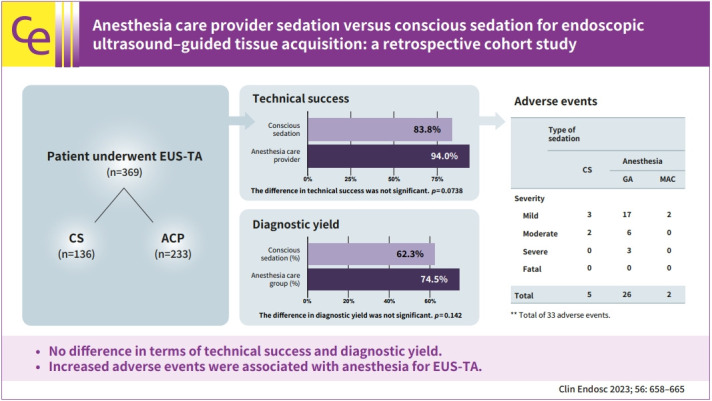
Results: Technical success was achieved in 219/233 (94.0%) in the ACP group and 114/136 (83.8%) in the CS group (p=0.0086). In multivariate analysis, the difference in technical success between the two groups was not significant (adjusted odds ratio [aOR], 0.5; 95% confidence interval [CI], 0.234-1.069; p=0.0738). A successful diagnostic yield was present in 146/196 (74.5%) in the ACP group and 66/106 (62.3%) in the CS group, respectively (p=0.0274). In multivariate analysis, the difference in diagnostic yield between the two groups was not significant (aOR, 0.643; 95% CI, 0.356-1.159; p=0.142). A total of 33 adverse events (AEs) were observed. The incidence of AEs was significantly lower in the CS group (5/33 CS vs. 28/33 ACP; OR, 0.281; 95% CI, 0.095-0.833; p=0.022).
Conclusion: CS provided equivalent technical success and diagnostic yield for malignancy in endoscopic ultrasound-guided tissue acquisition. Increased AEs were associated with anesthesia for the endoscopic ultrasound-guided tissue acquisition.
Keywords: Anesthesia; Conscious sedation; Endoscopic ultrasound–guided fine needle aspiration; General anesthesia.
Conflict of interest statement
The authors have no potential conflicts of interest.
Figures
Similar articles
-
Does general anesthesia increase the diagnostic yield of endoscopic ultrasound-guided fine needle aspiration of pancreatic masses?Anesthesiology. 2012 Nov;117(5):1044-50. doi: 10.1097/ALN.0b013e31826e0590. Anesthesiology. 2012. PMID: 23042221
-
Diagnostic Yield and Complications of EBUS-TBNA Performed Under Bronchoscopist-directed Conscious Sedation: Single Center Experience of 1004 Subjects.J Bronchology Interv Pulmonol. 2017 Jan;24(1):7-14. doi: 10.1097/LBR.0000000000000332. J Bronchology Interv Pulmonol. 2017. PMID: 27984382
-
Impact of Moderate Sedation versus Monitored Anesthesia Care on Outcomes and Cost of Endobronchial Ultrasound Transbronchial Needle Aspiration.Pulm Med. 2019 May 9;2019:4347852. doi: 10.1155/2019/4347852. eCollection 2019. Pulm Med. 2019. PMID: 31210988 Free PMC article.
-
Factors associated with diagnostic accuracy, technical success and adverse events of endoscopic ultrasound-guided fine-needle biopsy: A systematic review and meta-analysis.J Gastroenterol Hepatol. 2020 Aug;35(8):1264-1276. doi: 10.1111/jgh.14999. Epub 2020 Feb 23. J Gastroenterol Hepatol. 2020. PMID: 32003100
-
Endoscopic ultrasound guided fine needle aspiration and useful ancillary methods.World J Gastroenterol. 2014 Oct 21;20(39):14292-300. doi: 10.3748/wjg.v20.i39.14292. World J Gastroenterol. 2014. PMID: 25339816 Free PMC article. Review.
References
-
- Wani S, Muthusamy VR, Komanduri S. EUS-guided tissue acquisition: an evidence-based approach (with videos) Gastrointest Endosc. 2014;80:939–959. - PubMed
-
- Chen G, Liu S, Zhao Y, et al. Diagnostic accuracy of endoscopic ultrasound-guided fine-needle aspiration for pancreatic cancer: a meta-analysis. Pancreatology. 2013;13:298–304. - PubMed
-
- Thornton GD, McPhail MJ, Nayagam S, et al. Endoscopic ultrasound guided fine needle aspiration for the diagnosis of pancreatic cystic neoplasms: a meta-analysis. Pancreatology. 2013;13:48–57. - PubMed
-
- Siddiqui AA, Brown LJ, Hong SK, et al. Relationship of pancreatic mass size and diagnostic yield of endoscopic ultrasound-guided fine needle aspiration. Dig Dis Sci. 2011;56:3370–3375. - PubMed
LinkOut - more resources
Full Text Sources
