

Anxiety disorders across middle childhood and early adolescence in a UK population-based cohort
- PMID: 37431383
- PMCID: PMC10242895
- DOI: 10.1002/jcv2.12089
Anxiety disorders across middle childhood and early adolescence in a UK population-based cohort
Abstract
Background: Patterns of development and underlying factors explaining anxiety disorders in children and adolescents are under-researched, despite their high prevalence, impact and associations with other mental disorders. We aimed to a] understand the pattern and persistence of specific anxiety disorders; b] examine differing trajectories of symptoms of specific anxiety disorders and; c] examine socio-demographic and health-related predictors of persistent anxiety disorder-specific symptoms, across middle childhood to early adolescence.
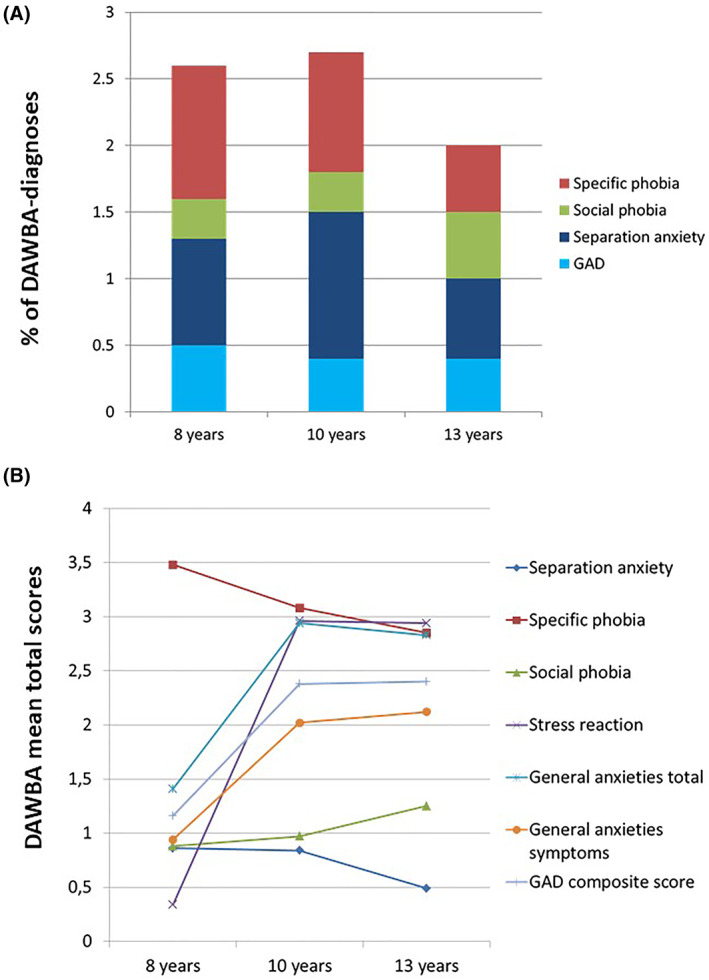
Methods: The current study used data from 8122 participants in the Avon Longitudinal Study of Parents and Children birth cohort. The Development and Wellbeing Assessment questionnaire was administered to parents to capture child and adolescent anxiety total scores and DAWBA-derived diagnoses. Separation anxiety, specific phobia, social anxiety, acute stress reaction, and generalized anxiety at 8, 10 and 13 years were selected. Further, we included the following socio-demographic and health-related predictors: sex, birth weight, sleep difficulties at 3.5 years, ethnicity, family adversity, maternal age at birth, maternal postnatal anxiety, maternal postnatal depression, maternal bonding, maternal socio-economic status and maternal education.
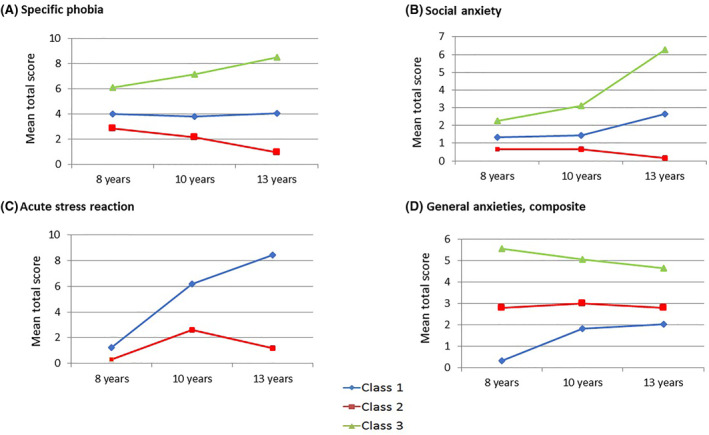
Results: Different anxiety disorders presented different prevalence and patterns of development over time. Further, latent class growth analyses yielded a trajectory characterized by individuals with persistent high levels of anxiety across childhood and adolescence; for specific phobia (high = 5.8%; moderate = 20.5%; low = 73.6%), social anxiety (high = 3.4%; moderate = 12.1%; low = 84.5%), acute stress reaction (high = 1.9%; low = 98.1%) and generalized anxiety (high = 5.4%; moderate = 21.7%; low = 72.9%). Finally, the risk factors associated with each of the persistent high levels of anxiety disorders were child sleeping difficulties and postnatal maternal depression and anxiety.
Conclusions: Our findings show that a small group of children and young adolescents continue to suffer from frequent and severe anxiety. When considering treatment strategies for anxiety disorders in this group, children's sleep difficulties and postnatal maternal depression and anxiety need to be assessed as these may predict a more prolonged and severe course of illness.
Keywords: ALSPAC; anxiety disorders; early adolescence; trajectories.
© 2022 The Authors. JCPP Advances published by John Wiley & Sons Ltd on behalf of Association for Child and Adolescent Mental Health.
Conflict of interest statement
The authors have declared that they have no competing or potential conflicts of interest.
Figures
References
-
- Achenbach, T. M. , Howell, C. T. , McConaughy, S. H. , & Stanger, C. (1998). Six‐year predictors of problems in a national sample: IV. Young adult signs of disturbance. Journal of the American Academy of Child & Adolescent Psychiatry, 37(7), 718–727. - PubMed
-
- Beesdo‐Baum, K. , & Knappe, S. (2012). Developmental epidemiology of anxiety disorders. Child and Adolescent Psychiatric Clinics, 21(3), 457–478. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources