

Early neurodevelopmental problems and risk for avoidant/restrictive food intake disorder (ARFID) in 4-7-year-old children: A Japanese birth cohort study
- PMID: 37431388
- PMCID: PMC10242837
- DOI: 10.1002/jcv2.12094
Early neurodevelopmental problems and risk for avoidant/restrictive food intake disorder (ARFID) in 4-7-year-old children: A Japanese birth cohort study
Abstract
Background: An overrepresentation of neurodevelopmental problems (NDPs) has been observed in individuals with avoidant/restrictive food intake disorder (ARFID). Previous studies on the association between ARFID and NDPs have been limited by cross-sectional data from clinical samples of small size. This study aimed to extend previous research by using prospectively collected data in a non-clinical child cohort. We examined the occurrence of early NDPs in 4-7-year-old children with suspected ARFID and how predictive early NDPs are of ARFID.
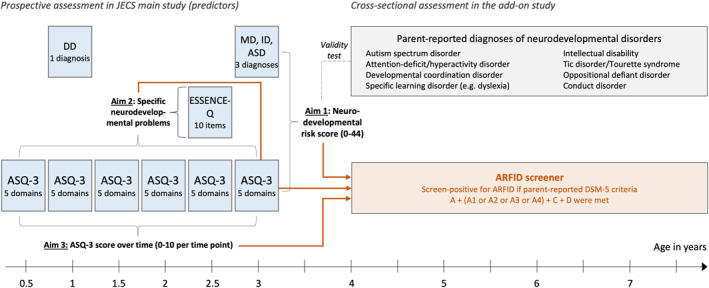
Methods: Data were collected via parent-report a sub-sample of the Japan Environment and Children's Study (JECS) including 3728 children born 2011-2014 in Kochi prefecture. NDPs were assessed biannually between 0.5 and 3 years of age with the Ages and Stages Questionnaire-3, at age 2.5 years with the ESSENCE-Q, and at age 1 and 3 years via parent-reported clinical diagnoses. ARFID was identified cross-sectionally (at age 4-7 years) using a newly developed screening tool. Logistic regressions were used to test association of (1) a composite early NDP risk score, (2) specific early NDPs, and (3) neurodevelopmental trajectories over time with ARFID.
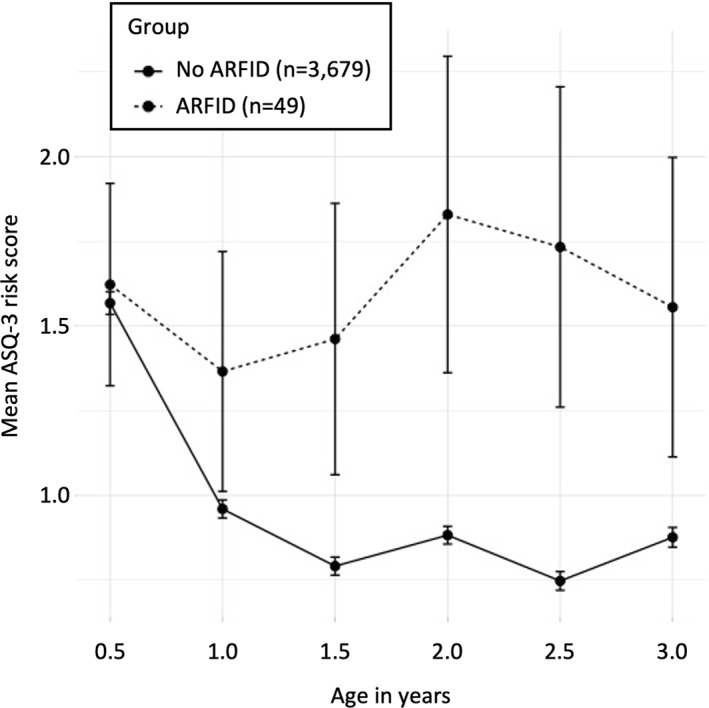
Results: Children in the highest risk percentiles of the NDP risk score had roughly three times higher odds of having suspected ARFID; the absolute risk of later ARFID for children above the 90th percentile was 3.1%. Early NDPs (excluding early feeding problems) were more predictive of later ARFID than were early feeding problems. Specific NDPs predictive of ARFID were problems with general development, communication/language, attention/concentration, social interaction, and sleep. Neurodevelopmental trajectories of children with and without suspected ARFID started to divert after age 1 year.
Conclusions: The results mirror the previously observed overrepresentation of NDPs in ARFID populations. In this non-clinical child cohort, early feeding problems were common and rarely developed into ARFID; however, our findings imply that they should be monitored closely in children with high NDP risk to prevent ARFID.
Keywords: Japan Environment and Children's Study (JECS); attention‐deficit/hyperactivity disorder; autism spectrum disorder; eating disorder; neurodevelopmental disorders.
© 2022 The Authors. JCPP Advances published by John Wiley & Sons Ltd on behalf of Association for Child and Adolescent Mental Health.
Conflict of interest statement
The authors have declared that they have no competing or potential conflicts of interest.
Figures
Similar articles
-
Development of a parent-reported screening tool for avoidant/restrictive food intake disorder (ARFID): Initial validation and prevalence in 4-7-year-old Japanese children.Appetite. 2022 Jan 1;168:105735. doi: 10.1016/j.appet.2021.105735. Epub 2021 Oct 6. Appetite. 2022. PMID: 34626753
-
The Polish Version of the Avoidant/Restrictive Food Intake Disorder Questionnaire-Parents Report (ARFID-Q-PR) and the Nine Items Avoidant/Restrictive Food Intake Disorder Screen-Parents Report (NIAS-PR): Maternal Perspective.Nutrients. 2022 Aug 2;14(15):3175. doi: 10.3390/nu14153175. Nutrients. 2022. PMID: 35956354 Free PMC article.
-
Birth-related, medical, and diagnostic characteristics in younger versus older children with avoidant/restrictive food intake disorder (ARFID).J Eat Disord. 2023 Oct 26;11(1):190. doi: 10.1186/s40337-023-00908-7. J Eat Disord. 2023. PMID: 37885020 Free PMC article.
-
Avoidant restrictive food intake disorder: recent advances in neurobiology and treatment.J Eat Disord. 2024 Jun 7;12(1):74. doi: 10.1186/s40337-024-01021-z. J Eat Disord. 2024. PMID: 38849953 Free PMC article. Review.
-
Delayed avoidant restrictive food intake disorder diagnosis leading to Ogilvie's syndrome in an adolescent.Eat Weight Disord. 2022 Jun;27(5):1913-1918. doi: 10.1007/s40519-021-01315-0. Epub 2021 Oct 8. Eat Weight Disord. 2022. PMID: 34623607 Review.
Cited by
-
The Co-Occurrence of Autism and Avoidant/Restrictive Food Intake Disorder (ARFID): A Prevalence-Based Meta-Analysis.Int J Eat Disord. 2025 Mar;58(3):473-488. doi: 10.1002/eat.24369. Epub 2025 Jan 6. Int J Eat Disord. 2025. PMID: 39760303 Free PMC article.
-
Physical health complications in children and young people with avoidant restrictive food intake disorder (ARFID): a systematic review and meta-analysis.BMJ Paediatr Open. 2024 Jul 8;8(1):e002595. doi: 10.1136/bmjpo-2024-002595. BMJ Paediatr Open. 2024. PMID: 38977355 Free PMC article.
-
Co-existing mental and somatic conditions in Swedish children with the avoidant restrictive food intake disorder phenotype.medRxiv [Preprint]. 2024 Mar 15:2024.03.10.24304003. doi: 10.1101/2024.03.10.24304003. medRxiv. 2024. Update in: JAMA Pediatr. 2025 Apr 01;179(4):428-437. doi: 10.1001/jamapediatrics.2024.6065. PMID: 38558975 Free PMC article. Updated. Preprint.
-
Neurodevelopmental and psychiatric conditions in 600 Swedish children with the avoidant/restrictive food intake disorder phenotype.J Child Psychol Psychiatry. 2025 Sep;66(9):1333-1344. doi: 10.1111/jcpp.14134. Epub 2025 Mar 12. J Child Psychol Psychiatry. 2025. PMID: 40074527 Free PMC article.
-
Symptoms of Avoidant/Restrictive Food Intake Disorder among 2-10-Year-Old Children: The Significance of Maternal Feeding Style and Maternal Eating Disorders.Nutrients. 2022 Oct 27;14(21):4527. doi: 10.3390/nu14214527. Nutrients. 2022. PMID: 36364790 Free PMC article.
References
-
- American Psychiatric Association . (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Association.
-
- Benjamini, Y. , & Hochberg, Y. (1995). Controlling the false discovery rate ‐ a practical and powerful approach to multiple testing. Journal of the Royal Statistical Society ‐ Series B: Statistical Methodology, 57(1), 289–300. 10.1111/j.2517-6161.1995.tb02031.x - DOI
-
- Benjamini, Y. , & Yekutieli, D. (2001). The control of the false discovery rate in multiple testing under dependency. Annals of Statistics, 29(4), 1165–1188. 10.1214/aos/1013699998 - DOI
LinkOut - more resources
Full Text Sources