

Treatment of Peri-Invagination Lesion and Vitality Preservation in Type III Dens Invaginatus in Bilateral Immature Maxillary Lateral Incisors: A Case Report
- PMID: 37431525
- PMCID: PMC10329757
- DOI: 10.22037/iej.v18i3.42102
Treatment of Peri-Invagination Lesion and Vitality Preservation in Type III Dens Invaginatus in Bilateral Immature Maxillary Lateral Incisors: A Case Report
Abstract
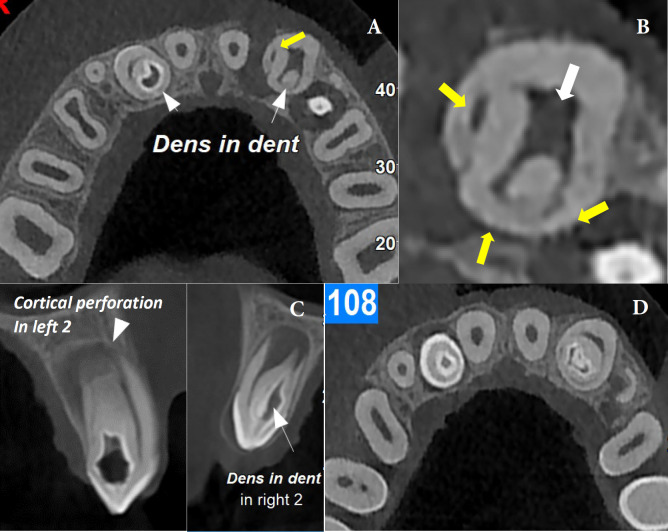
The superior lateral incisors are primarily affected by the developmental deformity known as dens invaginatus (DI). Oehler's type III DI has the highest complexity rendering a root canal treatment (RCT) an arduous challenge for this type, so early diagnosis and treatment before pulp involvement are important. This report presents two maxillary lateral incisors with type IIIb DI, the left one being associated with a periapical lesion and the right one with normal pulp. A nine-year-old boy was referred to our clinic complaining of mobility of the maxillary left lateral incisor (LLI) associated with gumboil throughout the previous two months. Periapical radiolucency was visible on radiographs, as well as an invagination that crosses the apical foramen from the pulp chamber in both maxillary lateral incisors. The pulp of the main canal of LLI was vital and pseudo canals were necrotized and associated with chronic apical abscess. Based on the condition of the main pulp of maxillary lateral incisors, two separate treatments were carried out. RCT was done only for the pseudo canals in the LLI, while the main root canal was preserved. The right maxillary lateral incisor (RLI) had vital pulp with normal periapical tissue So the invagination was sealed as the tooth was erupting. During the one-year follow-up period, the development of the root in LLI with a thick root wall and closed apex was observed in the periapical radiograph but pseudo canals became infected and the tooth became symptomatic, therefore retreatment for pseudo canals was carried out. The RLI root was developed and the tooth was clinically asymptomatic, so it didn't need further treatment. Maintaining pulp vitality is crucial for type III Dens invaginated young permanent teeth since it could support root formation and improve long-term prognosis, and in cases with pulp involvement, non-surgical RCT is clinically predictable.
Keywords: Cone-beam Computed Tomography; Dens Invaginatus; Endodontic Treatment; Immature Permanent Teeth; Maxillary Lateral Incisors.
Conflict of interest statement
‘None declared’.
Figures



References
-
- Alani A, Bishop K. Dens invaginatus Part 1: classification, prevalence and aetiology. Int Endod J. 2008;41(12):1123–36. - PubMed
-
- Hülsmann M. Dens invaginatus: aetiology, classification, prevalence, diagnosis, and treatment considerations. Int Endod J. 1997;30(2):79–90. - PubMed
-
- Monteiro-Jardel CC, Alves FR. Type III dens invaginatus in a mandibular incisor: a case report of a conventional endodontic treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;111(4):e29–32. - PubMed
-
- Zhang P, Wei X. Combined Therapy for a Rare Case of Type III Dens Invaginatus in a Mandibular Central Incisor with a Periapical Lesion: A Case Report. J Endod. 2017;43(8):1378–82. - PubMed
-
- Zhu J, Wang X, Fang Y, Von den Hoff JW, Meng L. An update on the diagnosis and treatment of dens invaginatus. Aust Dent J. 2017;62(3):261–75. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous