

Rare Forms of Cardiac Amyloidosis: Diagnostic Clues and Phenotype in Apo AI and AIV Amyloidosis
- PMID: 37431665
- PMCID: PMC10351905
- DOI: 10.1161/CIRCIMAGING.123.015259
Rare Forms of Cardiac Amyloidosis: Diagnostic Clues and Phenotype in Apo AI and AIV Amyloidosis
Abstract
Background: Apo AI amyloidosis (AApoAI) and Apo AIV amyloidosis (AApoAIV) are rare but increasingly recognized causes of cardiac amyloidosis (CA). We sought to define the cardiac phenotype in AApoAI and AApoAIV using multimodality imaging.
Methods: We identified all patients with AApoAI and AApoAIV assessed at our center between 2000 and 2021, and 2 cohorts of patients with immunoglobulin light-chain amyloidosis (AL) and transthyretin amyloidosis matched for age, sex, and cardiac involvement.
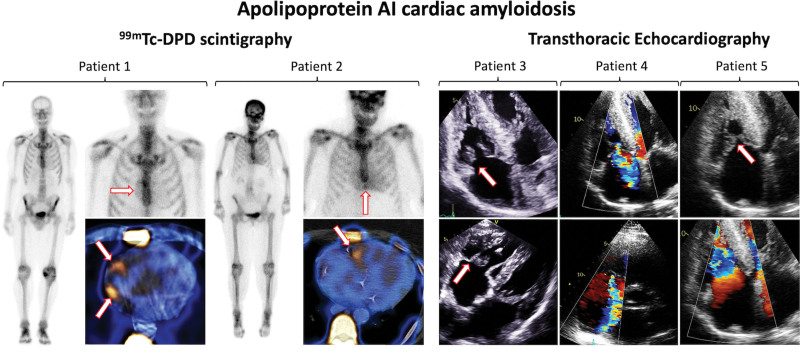
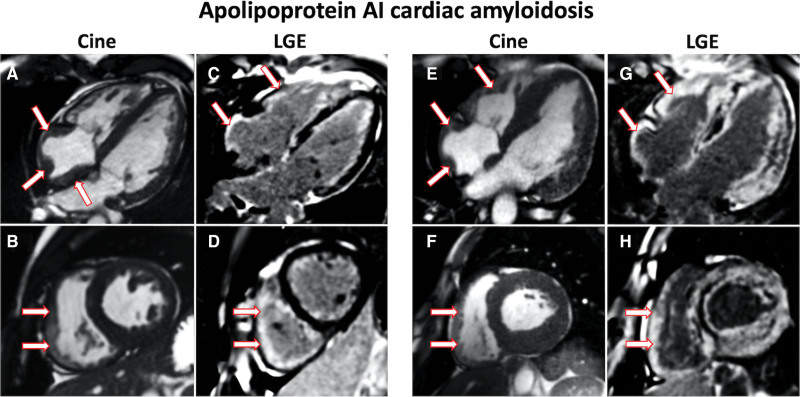
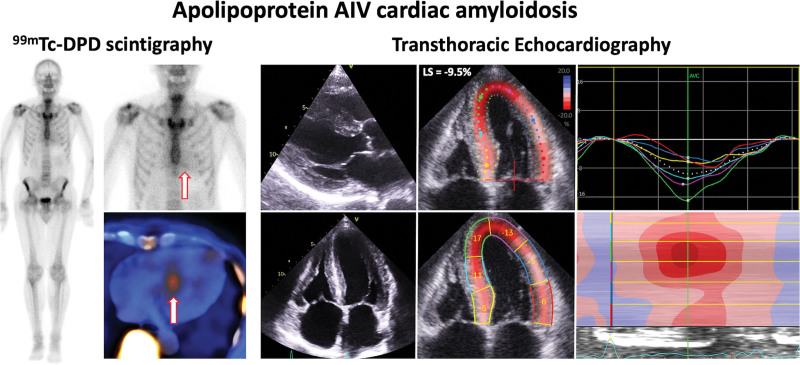
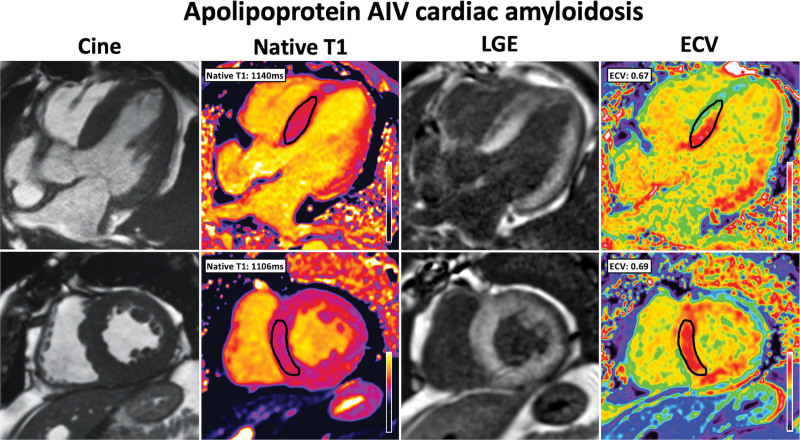
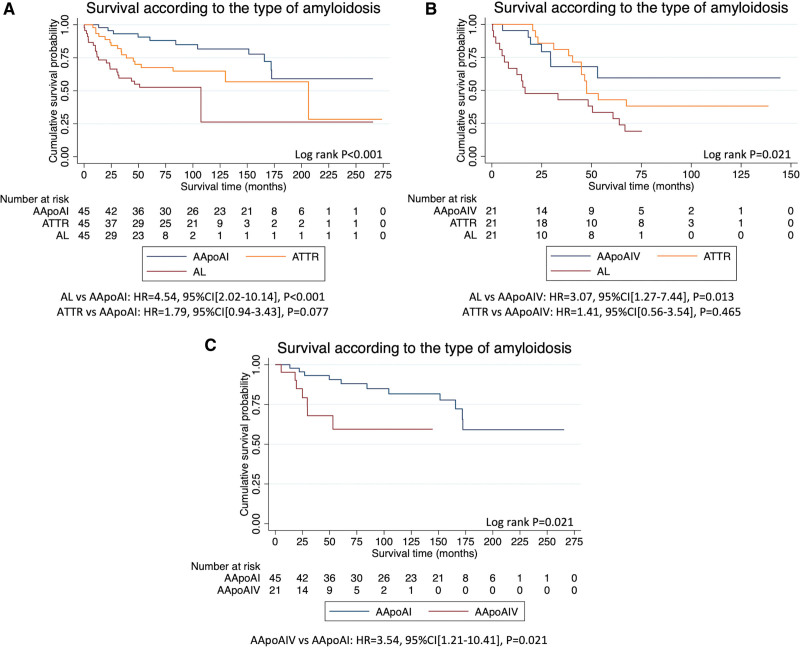
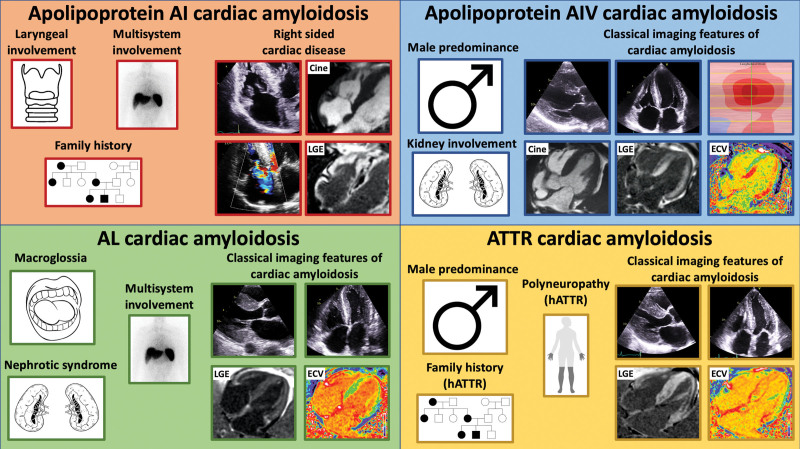
Results: Forty-five patients had AApoAI, 13 (29%) of whom had cardiac involvement, 32 (71%) renal involvement, 28 (62%) splenic involvement, 27 (60%) hepatic involvement, and 7 (16%) laryngeal involvement. AApoAI-CA commonly presented with heart failure (n=8, 62%) or dysphonia (n=7, 54%). The Arg173Pro variant universally caused cardiac and laryngeal involvement (n=7, 100%). AApoAI-CA was associated with right-sided involvement, with a thicker right ventricular free wall (8.6±1.9 versus 6.3±1.3 mm versus 7.7±1.2 mm, P=0.004), greater incidence of tricuspid stenosis (4 [31%] versus 0 [0%] versus 0 [0%], P=0.012) and tricuspid regurgitation (6 [46%] versus 1 [8%] versus 2 [15%], P=0.048) than AL-CA and transthyretin CA. Twenty-one patients had AApoAIV, and cardiac involvement was more common than in AApoAI (15 [71%] versus 13 [29%], P=0.001). AApoAIV-CA most commonly presented with heart failure (n=12, 80%), and a lower median estimated glomerular filtration rate than AL-CA and transthyretin CA (36 mL/[min·1.73 m²] versus 65 mL/[min·1.73 m²] versus 63 mL/[min·1.73 m²], P<0.001). All AApoAIV-CA patients had classical CA features on echocardiography/cardiac magnetic resonance, including an apical-sparing strain pattern, which was less common in AApoAI-CA (15 [100%] versus 7 [54%], P=0.003), whereas cardiac uptake on bone scintigraphy was less common in AApoAIV-CA than AApoAI-CA (all grade 1) (14% versus 82%, P<0.001). Patients with AApoAI and AApoAIV had a good prognosis (median survival >172 and >30 months, respectively), and a lower risk of mortality than matched patients with AL-amyloidosis (AL versus AApoAI: hazard ratio, 4.54 [95% CI, 2.02-10.14]; P<0.001; AL versus AApoAIV: hazard ratio, 3.07 [95% CI, 1.27-7.44]; P=0.013).
Conclusions: Dysphonia, multisystem involvement, or right-sided cardiac disease should raise suspicion of AApoAI-CA. AApoAIV-CA presents most commonly with heart failure and always displays classical CA imaging features, mimicking common forms of CA. Both AApoAI and AApoAIV are associated with a good prognosis and a lower risk of mortality than matched patients with AL-amyloidosis.
Keywords: amyloidosis; apolipoprotein; hereditary; phenotype; prognosis; transthyretin-related.
Conflict of interest statement
Figures
References
-
- Wechalekar AD, Gillmore JD, Hawkins PN. Systemic amyloidosis. Lancet. 2016;387:2641–2654. doi: 10.1016/S0140-6736 (15) 01274-X - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
