

Sepsis-associated acute kidney injury in the intensive care unit: incidence, patient characteristics, timing, trajectory, treatment, and associated outcomes. A multicenter, observational study
- PMID: 37432520
- PMCID: PMC10499944
- DOI: 10.1007/s00134-023-07138-0
Sepsis-associated acute kidney injury in the intensive care unit: incidence, patient characteristics, timing, trajectory, treatment, and associated outcomes. A multicenter, observational study
Abstract
Purpose: The Acute Disease Quality Initiative (ADQI) Workgroup recently released a consensus definition of sepsis-associated acute kidney injury (SA-AKI), combining Sepsis-3 and Kidney Disease Improving Global Outcomes (KDIGO) AKI criteria. This study aims to describe the epidemiology of SA-AKI.
Methods: This is a retrospective cohort study carried out in 12 intensive care units (ICUs) from 2015 to 2021. We studied the incidence, patient characteristics, timing, trajectory, treatment, and associated outcomes of SA-AKI based on the ADQI definition.
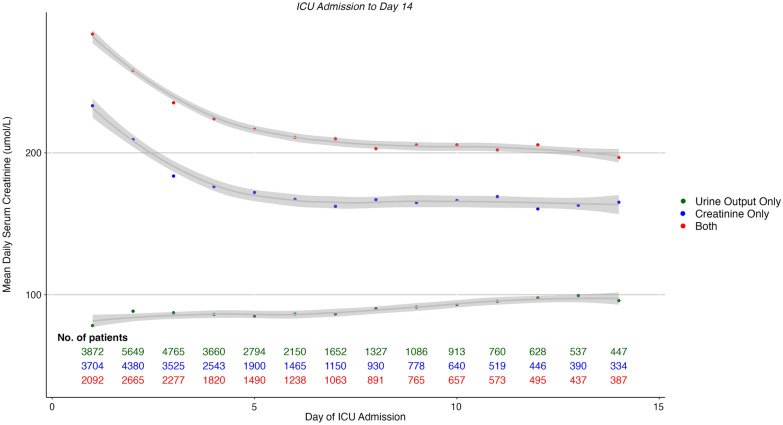
Results: Out of 84,528 admissions, 13,451 met the SA-AKI criteria with its incidence peaking at 18% in 2021. SA-AKI patients were typically admitted from home via the emergency department (ED) with a median time to SA-AKI diagnosis of 1 day (interquartile range (IQR) 1-1) from ICU admission. At diagnosis, most SA-AKI patients (54%) had a stage 1 AKI, mostly due to the low urinary output (UO) criterion only (65%). Compared to diagnosis by creatinine alone, or by both UO and creatinine criteria, patients diagnosed by UO alone had lower renal replacement therapy (RRT) requirements (2.8% vs 18% vs 50%; p < 0.001), which was consistent across all stages of AKI. SA-AKI hospital mortality was 18% and SA-AKI was independently associated with increased mortality. In SA-AKI, diagnosis by low UO only, compared to creatinine alone or to both UO and creatinine criteria, carried an odds ratio of 0.34 (95% confidence interval (CI) 0.32-0.36) for mortality.
Conclusion: SA-AKI occurs in 1 in 6 ICU patients, is diagnosed on day 1 and carries significant morbidity and mortality risk with patients mostly admitted from home via the ED. However, most SA-AKI is stage 1 and mostly due to low UO, which carries much lower risk than diagnosis by other criteria.
Keywords: Acute kidney injury; Critical care; Sepsis; Sepsis-associated acute kidney injury.
© 2023. The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Comment in
-
Clinical implications of urine output-based sepsis-associated acute kidney injury.Intensive Care Med. 2023 Oct;49(10):1263-1265. doi: 10.1007/s00134-023-07190-w. Epub 2023 Aug 21. Intensive Care Med. 2023. PMID: 37604956 No abstract available.
-
Double the risk of death and other 'inconvenient truths' about oliguria.Intensive Care Med. 2023 Nov;49(11):1420-1421. doi: 10.1007/s00134-023-07187-5. Epub 2023 Aug 24. Intensive Care Med. 2023. PMID: 37620560 No abstract available.
-
Tackling sepsis-associated acute kidney injury using routinely collected data.Intensive Care Med. 2023 Sep;49(9):1100-1102. doi: 10.1007/s00134-023-07200-x. Epub 2023 Aug 28. Intensive Care Med. 2023. PMID: 37638977 No abstract available.
-
Details and the devil within - the case of sepsis associated acute kidney injury.Intensive Care Med. 2023 Nov;49(11):1424-1425. doi: 10.1007/s00134-023-07204-7. Epub 2023 Aug 31. Intensive Care Med. 2023. PMID: 37650942 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
