

Non-demyelinating disorders mimicking and misdiagnosed as NMOSD: a literature review
- PMID: 37433584
- PMCID: PMC10530555
- DOI: 10.1111/ene.15983
Non-demyelinating disorders mimicking and misdiagnosed as NMOSD: a literature review
Abstract
Background: Differentiating neuromyelitis optica spectrum disorder (NMOSD) from its mimics is crucial to avoid misdiagnosis, especially in the absence of aquaporin-4-IgG. While multiple sclerosis (MS) and myelin oligodendrocyte glycoprotein-IgG associated disease (MOGAD) represent major and well-defined differential diagnoses, non-demyelinating NMOSD mimics remain poorly characterized.
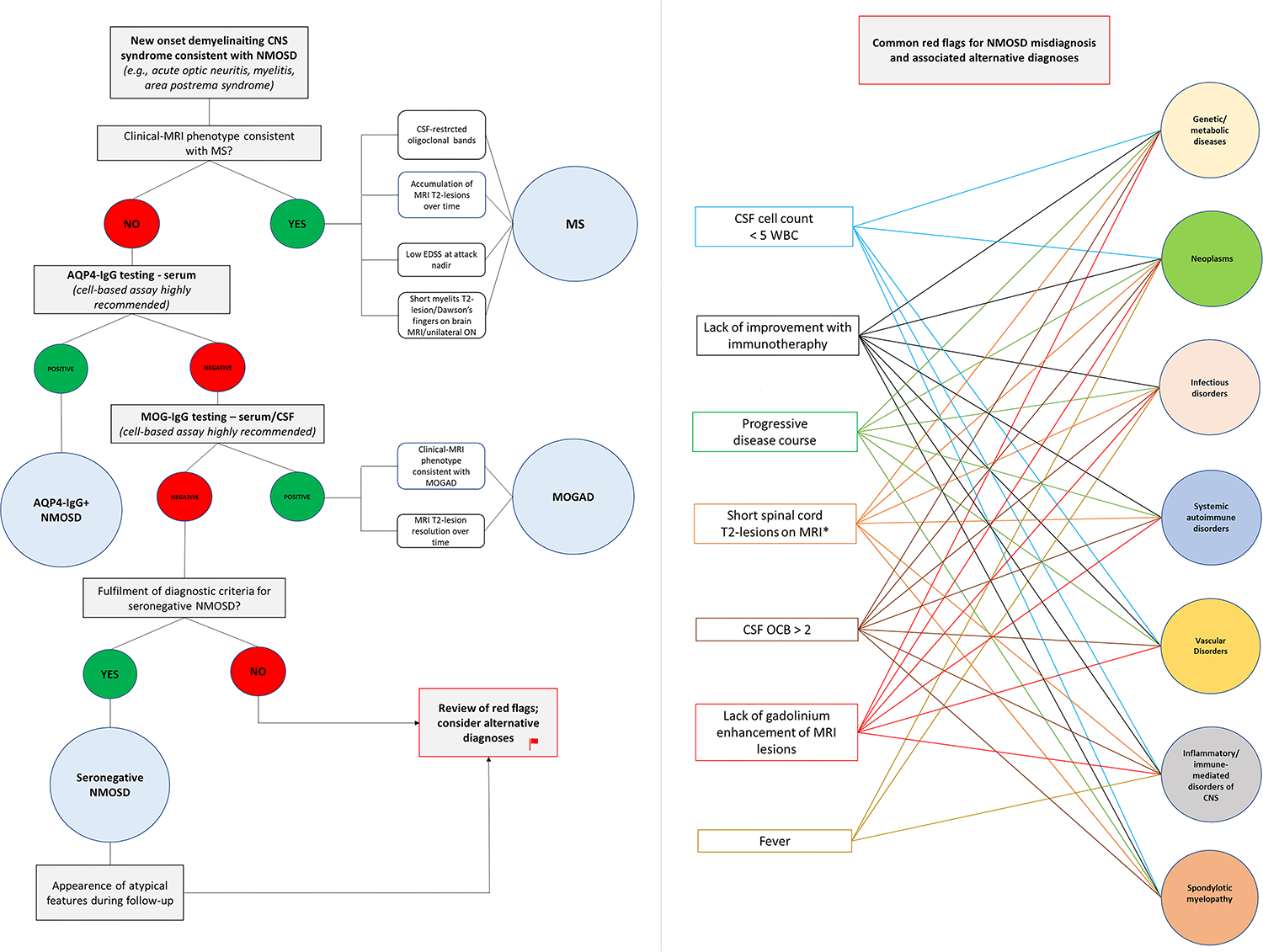
Methods: We conducted a systematic review on PubMed/MEDLINE to identify reports of patients with non-demyelinating disorders that mimicked or were misdiagnosed as NMOSD. Three novel cases seen at the authors' institutions were also included. The characteristics of NMOSD mimics were analyzed and red flags associated with misdiagnosis identified.
Results: A total of 68 patients were included; 35 (52%) were female. Median age at symptoms onset was 44 (range, 1-78) years. Fifty-six (82%) patients did not fulfil the 2015 NMOSD diagnostic criteria. The clinical syndromes misinterpreted for NMOSD were myelopathy (41%), myelopathy + optic neuropathy (41%), optic neuropathy (6%), or other (12%). Alternative etiologies included genetic/metabolic disorders, neoplasms, infections, vascular disorders, spondylosis, and other immune-mediated disorders. Common red flags associated with misdiagnosis were lack of cerebrospinal fluid (CSF) pleocytosis (57%), lack of response to immunotherapy (55%), progressive disease course (54%), and lack of magnetic resonance imaging gadolinium enhancement (31%). Aquaporin-4-IgG positivity was detected in five patients by enzyme-linked immunosorbent assay (n = 2), cell-based assay (n = 2: serum, 1; CSF, 1), and non-specified assay (n = 1).
Conclusions: The spectrum of NMOSD mimics is broad. Misdiagnosis frequently results from incorrect application of diagnostic criteria, in patients with multiple identifiable red flags. False aquaporin-4-IgG positivity, generally from nonspecific testing assays, may rarely contribute to misdiagnosis.
Keywords: differential diagnosis; false positivity; mimickers; misdiagnosis; neuromyelitis optica spectrum disorder.
© 2023 European Academy of Neurology.
Conflict of interest statement
Conflict of Interest Statement
Drs. Zara, Dinoto, Carta, Floris, and Turilli have nothing to disclose. Adrian Budhram reports that he holds the London Health Sciences Centre and London Health Sciences Foundation Chair in Neural Antibody Testing for Neuro-Inflammatory Diseases and receives support from the Opportunities Fund of the Academic Health Sciences Centre Alternative Funding Plan of the Academic Medical Organization of Southwestern Ontario (AMOSO). Sergio Ferrari received speaker honoraria from Lundbeck and support for scientific meeting by Shire, Merck, Euroimmun. Paolo Solla has received speaker honoraria from Bayer and Zambon. Sara Mariotto has received speaker honoraria from Biogen, Novartis, and Sanofy. Eoin P. Flanagan has served on advisory boards for Alexion, Genentech, Horizon Therapeutics and UCB. He has received research support from UCB. He has received speaker honoraria from Pharmacy Times. He received royalties from UpToDate. Dr Flanagan was a site primary investigator in a randomized clinical trial on Inebilizumab in neuromyelitis optica spectrum disorder run by Medimmune/Viela-Bio/Horizon Therapeutics. Dr Flanagan has received funding from the NIH (R01NS113828). Dr Flanagan is a member of the medical advisory board of the MOG project. Dr Flanagan is an editorial board member of the Journal of the Neurological Sciences and Neuroimmunology Reports. A patent has been submitted on DACH1-IgG as a biomarker of paraneoplastic autoimmunity. A Sebastian Lopez Chiriboga has served on scientific advisory boards for Genentech and Horizon. Elia Sechi has received speaker honoraria and support for attending scientific meetings from Alexion. He serves as an editorial board member for BMC Neurology and Frontiers in Neurology. Dr. Sechi is a member of the medical advisory board of the MOG project.
Figures

References
-
- Carnero Contentti E, Lopez PA, Criniti J, et al. Frequency of NMOSD misdiagnosis in a cohort from Latin America: Impact and evaluation of different contributors. Mult Scler 2023;29:277–286. - PubMed
-
- Smith AD, Moog TM, Burgess KW, McCreary M, Okuda DT. Factors associated with the misdiagnosis of neuromyelitis optica spectrum disorder. Mult Scler Relat Disord 2023;70:104498. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
