

Think out of the box: association of left congenital diaphragmatic hernia and abnormal origin of the right pulmonary artery : A train can hide another
- PMID: 37434143
- PMCID: PMC10334659
- DOI: 10.1186/s12887-023-04164-1
Think out of the box: association of left congenital diaphragmatic hernia and abnormal origin of the right pulmonary artery : A train can hide another
Abstract
Background: We report the occurrence of a severe pulmonary hypertension (PH) in a neonate affected by a left congenital diaphragmatic hernia (CDH). PH in this patient was associated with an abnormal origin of the right pulmonary artery from the right brachiocephalic artery. This malformation, sometimes named hemitruncus arteriosus, has to the best of our knowledge never been reported in association with a CDH.
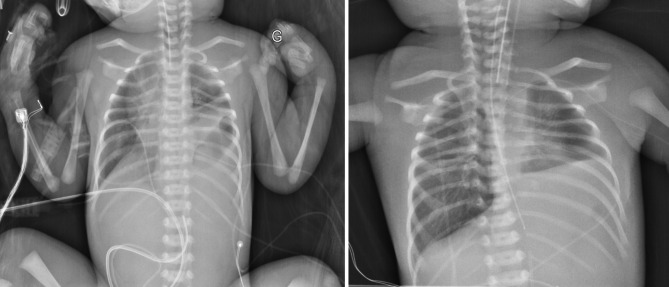
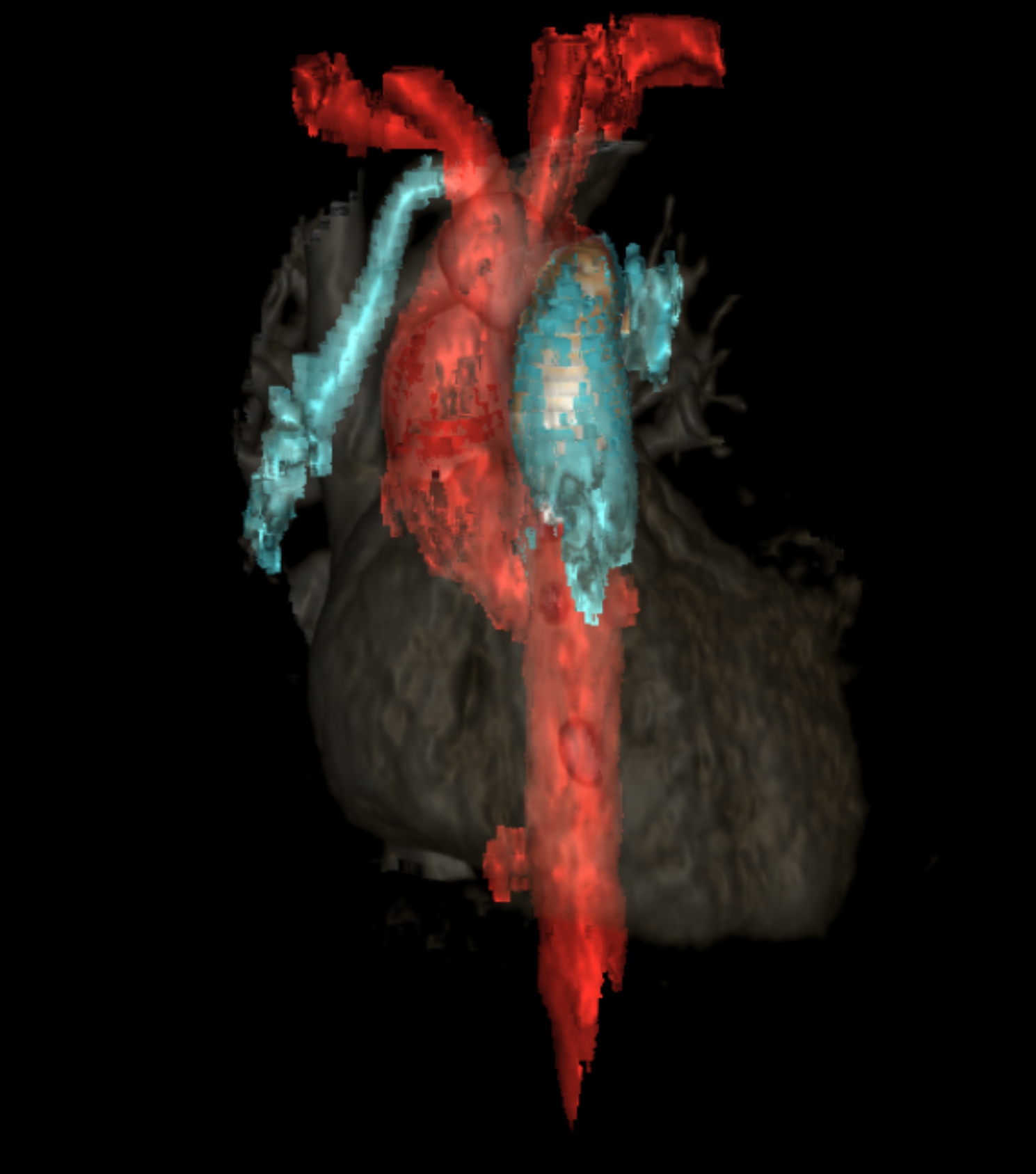
Case presentation: A male newborn was hospitalized from birth in the neonatal intensive care unit after prenatal diagnosis of a left CDH. Ultrasound examination at 34 weeks of gestational age evaluated the observed-to-expected lung-to-head ratio at 49%. Birth occurred at 38+ 5 weeks of gestational age. Soon after admission, severe hypoxemia, i.e., preductal pulse oximetry oxygen saturation (SpO2) < 80%, prompted therapeutic escalation including the use of high frequency oscillatory ventilation with fraction of inspired oxygen (FiO2) 100% and inhaled nitric oxide (iNO). Echocardiography assessment revealed signs of severe PH and normal right ventricle function. Despite administration of epoprostenolol, milrinone, norepinephrine, and fluid loadings with albumin and 0.9% saline, hypoxemia remained severe, preductal SpO2 inconsistently greater than or equal to 80-85% and post ductal SpO2 lower on average by 15 points. This clinical status remained unchanged during the first 7 days of life. The infant's clinical instability was incompatible with surgical intervention, while chest X-ray showed a relatively preserved lung volume, especially on the right side. This prompted an additional echocardiography, aimed at searching an explanation of this unusual evolution and found an abnormal origin of the right pulmonary artery, which was confirmed on computed tomography angiography subsequently. A change in the medical strategy was decided, with the suspension of pulmonary vasodilator treatments, the administration of diuretics, and the decrease in norepinephrine dose to decrease the systemic-to-pulmonary shunt. Progressive improvement in the infant respiratory and hemodynamic status enabled to perform CDH surgical repair 2 weeks after birth.
Conclusions: This case recalls the interest of systematic analysis of all potential causes of PH in a neonate with CDH, a condition frequently associated with various congenital malformations.
Keywords: Congenital diaphragmatic hernia; Congenital heart disease; Pediatrics; Poiseuille’s law; Pulmonary hypertension.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Differences in preductal and postductal arterial blood gas measurements in infants with severe congenital diaphragmatic hernia.Arch Dis Child Fetal Neonatal Ed. 2016 Jul;101(4):F314-8. doi: 10.1136/archdischild-2014-307714. Epub 2015 Oct 29. Arch Dis Child Fetal Neonatal Ed. 2016. PMID: 26514398
-
Safety and tolerability of subcutaneous treprostinil in newborns with congenital diaphragmatic hernia and life-threatening pulmonary hypertension.J Pediatr Surg. 2017 Sep;52(9):1480-1483. doi: 10.1016/j.jpedsurg.2017.03.058. Epub 2017 Mar 28. J Pediatr Surg. 2017. PMID: 28389079
-
Fetal ultrasound markers of severity predict resolution of pulmonary hypertension in congenital diaphragmatic hernia.Am J Obstet Gynecol. 2015 Aug;213(2):216.e1-8. doi: 10.1016/j.ajog.2015.03.036. Epub 2015 Mar 19. Am J Obstet Gynecol. 2015. PMID: 25797231 Free PMC article.
-
Management of pulmonary hypertension in infants with congenital diaphragmatic hernia.J Perinatol. 2016 Jun;36 Suppl 2:S28-31. doi: 10.1038/jp.2016.46. J Perinatol. 2016. PMID: 27225962 Review.
-
Neonatal and fetal therapy of congenital diaphragmatic hernia-related pulmonary hypertension.Arch Dis Child Fetal Neonatal Ed. 2022 Sep;107(5):458-466. doi: 10.1136/archdischild-2021-322617. Epub 2021 Dec 24. Arch Dis Child Fetal Neonatal Ed. 2022. PMID: 34952853 Review.
References
-
- Storme L, Boubnova J, Mur S, Pognon L, Sharma D, Aubry E et al. Review shows that implementing a nationwide protocol for congenital diaphragmatic hernia was a key factor in reducing mortality and morbidity. Acta Paediatr Oslo Nor 1992. 2018;107:1131–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
