

Infrarenal inferior vena cava agenesis presenting as acute abdomen and hydronephrosis - case report
- PMID: 37434616
- PMCID: PMC10331014
- DOI: 10.1016/j.radcr.2023.06.003
Infrarenal inferior vena cava agenesis presenting as acute abdomen and hydronephrosis - case report
Abstract
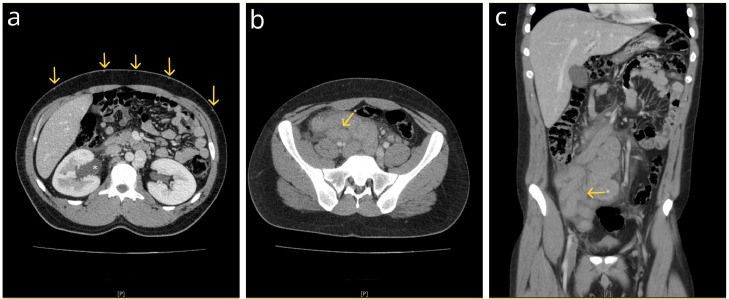
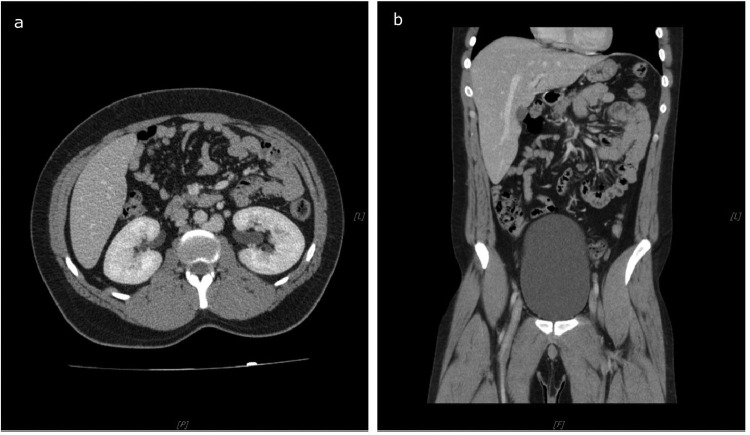
The inferior vena cava agenesis (IVCA) is a rare and often asymptomatic malformation due to the abundant development of the collateral circulation. However, it is frequently found in young people and carries a significant risk of deep venous thrombosis (DVT). It is estimated that about 5% of patients under 30 years of age presenting with DVT have this condition. We report a case of a previously healthy 23-year-old patient presenting with signs of acute abdomen and hydronephrosis due to the thrombophlebitis of an unusual iliocaval venous collateral, which developed secondary to IVCA. After treatment, the iliocaval collateral and hydronephrosis completely regressed on a 1-year follow-up. To our knowledge, this is the first such case reported in the literature.
Keywords: Acute abdomen; Collateral vein; Deep vein thrombosis; Hydronephrosis; Inferior vena cava agenesis; Thrombophlebitis.
© 2023 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures



References
-
- Tucker WD, Shrestha R, Anatomy Burns B. StatPearls. StatPearls Publishing; Treasure Island (FL): 2023. Abdomen and pelvis: inferior vena cava.https://www.ncbi.nlm.nih.gov/books/NBK482353/ [accessed July 25, 2022] - PubMed
-
- Gensas CS, Pires LM, Kruse ML, Leiria TL, Gomes DG, Lima GG. Agenesis of the inferior vena cava. Rev Bras de Cardiol Invasiva (English Edition) 2012;20(no. 4):427–430. doi: 10.1016/S2214-1235(15)30090-9. - DOI
-
- Knipp B, Knechtges P, Gest T, Wakefield T. Inferior vena cava: embryology and anomalies. Aortic Aneurysms. 2009;1:289–307. doi: 10.1007/978-1-60327-204-9_20. - DOI
Publication types
LinkOut - more resources
Full Text Sources
