

Ethnic differences in the indirect effects of the COVID-19 pandemic on clinical monitoring and hospitalisations for non-COVID conditions in England: a population-based, observational cohort study using the OpenSAFELY platform
- PMID: 37434746
- PMCID: PMC10331810
- DOI: 10.1016/j.eclinm.2023.102077
Ethnic differences in the indirect effects of the COVID-19 pandemic on clinical monitoring and hospitalisations for non-COVID conditions in England: a population-based, observational cohort study using the OpenSAFELY platform
Abstract
Background: The COVID-19 pandemic disrupted healthcare and may have impacted ethnic inequalities in healthcare. We aimed to describe the impact of pandemic-related disruption on ethnic differences in clinical monitoring and hospital admissions for non-COVID conditions in England.
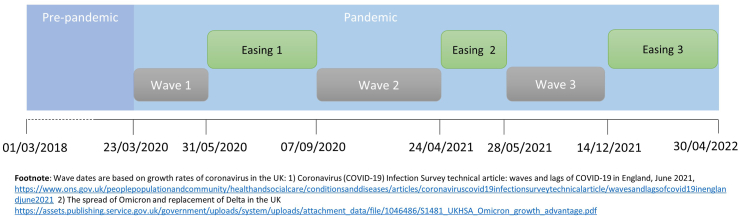
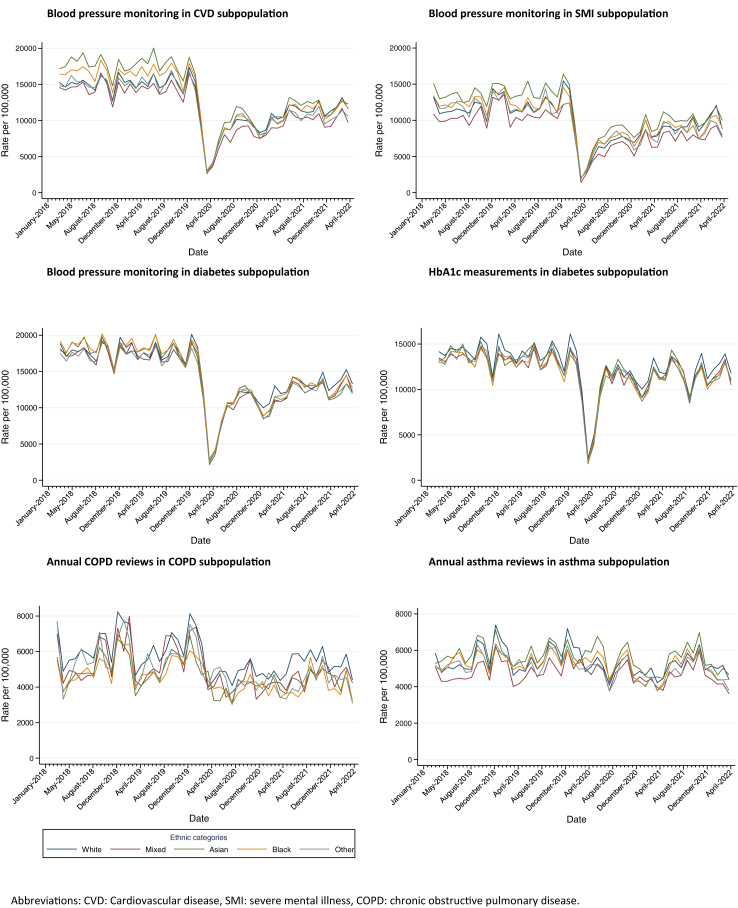
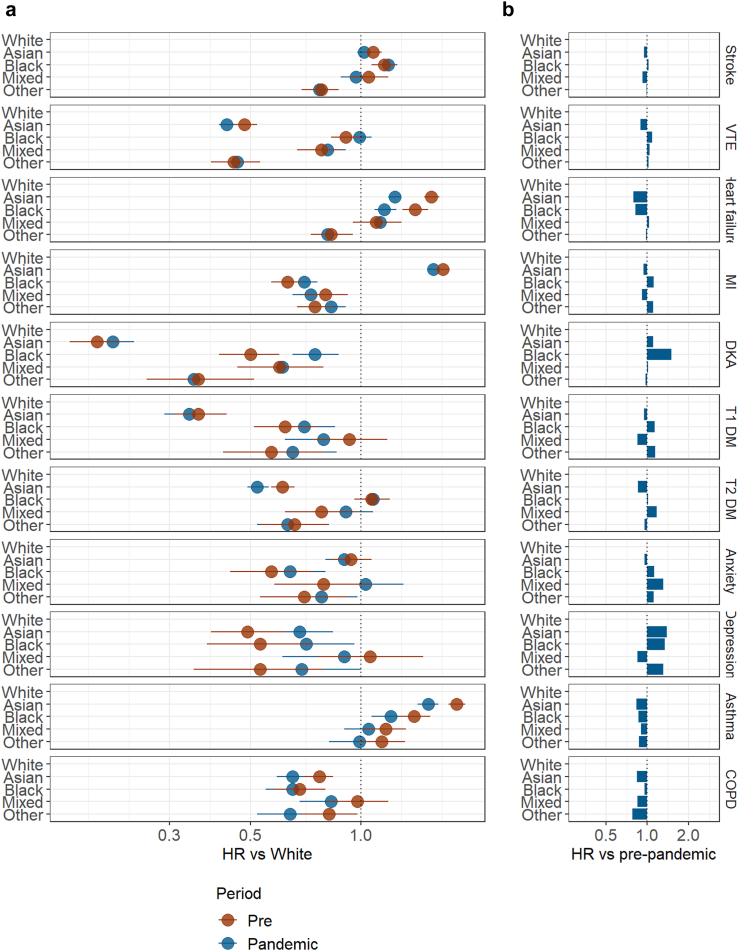
Methods: In this population-based, observational cohort study we used primary care electronic health record data with linkage to hospital episode statistics data and mortality data within OpenSAFELY, a data analytics platform created, with approval of NHS England, to address urgent COVID-19 research questions. We included adults aged 18 years and over registered with a TPP practice between March 1, 2018, and April 30, 2022. We excluded those with missing age, sex, geographic region, or Index of Multiple Deprivation. We grouped ethnicity (exposure), into five categories: White, Asian, Black, Other, and Mixed. We used interrupted time-series regression to estimate ethnic differences in clinical monitoring frequency (blood pressure and Hba1c measurements, chronic obstructive pulmonary disease and asthma annual reviews) before and after March 23, 2020. We used multivariable Cox regression to quantify ethnic differences in hospitalisations related to diabetes, cardiovascular disease, respiratory disease, and mental health before and after March 23, 2020.
Findings: Of 33,510,937 registered with a GP as of 1st January 2020, 19,064,019 were adults, alive and registered for at least 3 months, 3,010,751 met the exclusion criteria and 1,122,912 were missing ethnicity. This resulted in 14,930,356 adults with known ethnicity (92% of sample): 86.6% were White, 7.3% Asian, 2.6% Black, 1.4% Mixed ethnicity, and 2.2% Other ethnicities. Clinical monitoring did not return to pre-pandemic levels for any ethnic group. Ethnic differences were apparent pre-pandemic, except for diabetes monitoring, and remained unchanged, except for blood pressure monitoring in those with mental health conditions where differences narrowed during the pandemic. For those of Black ethnicity, there were seven additional admissions for diabetic ketoacidosis per month during the pandemic, and relative ethnic differences narrowed during the pandemic compared to the White ethnic group (Pre-pandemic hazard ratio (HR): 0.50, 95% confidence interval (CI) 0.41, 0.60, Pandemic HR: 0.75, 95% CI: 0.65, 0.87). There was increased admissions for heart failure during the pandemic for all ethnic groups, though highest in those of White ethnicity (heart failure risk difference: 5.4). Relatively, ethnic differences narrowed for heart failure admission in those of Asian (Pre-pandemic HR 1.56, 95% CI 1.49, 1.64, Pandemic HR 1.24, 95% CI 1.19, 1.29) and Black ethnicity (Pre-pandemic HR 1.41, 95% CI: 1.30, 1.53, Pandemic HR: 1.16, 95% CI 1.09, 1.25) compared with White ethnicity. For other outcomes the pandemic had minimal impact on ethnic differences.
Interpretation: Our study suggests that ethnic differences in clinical monitoring and hospitalisations remained largely unchanged during the pandemic for most conditions. Key exceptions were hospitalisations for diabetic ketoacidosis and heart failure, which warrant further investigation to understand the causes.
Funding: LSHTM COVID-19 Response Grant (DONAT15912).
Keywords: Ethnic differences; Healthcare utilisation; Pandemic.
© 2023 The Authors.
Conflict of interest statement
SVK was co-chair of the Scottish Government's Expert Reference Group on Ethnicity and COVID-19 and a member of the Scientific Advisory Group on Emergencies (SAGE) subgroup on ethnicity. RM and RME were members of the SAGE subgroup on ethnicity. REC has personal shares in AstraZeneca (AZ) unrelated to this work. BMK is also employed by NHS England (all declarations are openly available at: https://www.whopaysthisdoctor.org/doctor/491/active). JFH has grant funding from UKRI and the Wellcome Trust, has a patent with Juli Health unrelated to this work and has received consultancy fees from Juli Health and the Wellcome Trust unrelated to this work. RM is supported by Barts Charity (MGU0504), receives salary contributions from Genes & Health and has received consultancy fees from AMGEN. JKQ has grants from MRC, HDR UK, GlaxoSmithKline (GSK), BI, asthma + lung UK, and AZ and has received fees from GSK, Evidera, AZ and Insmed. SL was co-founder and co-chair of the RECORD steering committee and has a leadership role at Health Data Research UK. KM has received consultancy fees from AMGEN. LT has grant funding from MRC, the Wellcome Trust and is funded by an NIHR Research Professorship (NIHR302405), has consulted for Bayer and is on the MHRA expert advisory group (Women's health) and a member of 4 non-industry funded trial advisory committees (unpaid). All other authors declare no competing interests. AM has received consultancy fees from induction health and is a member of RCGP health informatics group and the NHS Digital GP data Professional Advisory Group.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
