

Correlation of Common Carotid Artery Blood Flow Parameters With Transthoracic Echocardiographic Cardiac Output for Assessing Fluid Responsiveness After Passive Leg Raising (PLR) Test in Critically Ill Patients
- PMID: 37435241
- PMCID: PMC10332793
- DOI: 10.7759/cureus.40229
Correlation of Common Carotid Artery Blood Flow Parameters With Transthoracic Echocardiographic Cardiac Output for Assessing Fluid Responsiveness After Passive Leg Raising (PLR) Test in Critically Ill Patients
Abstract
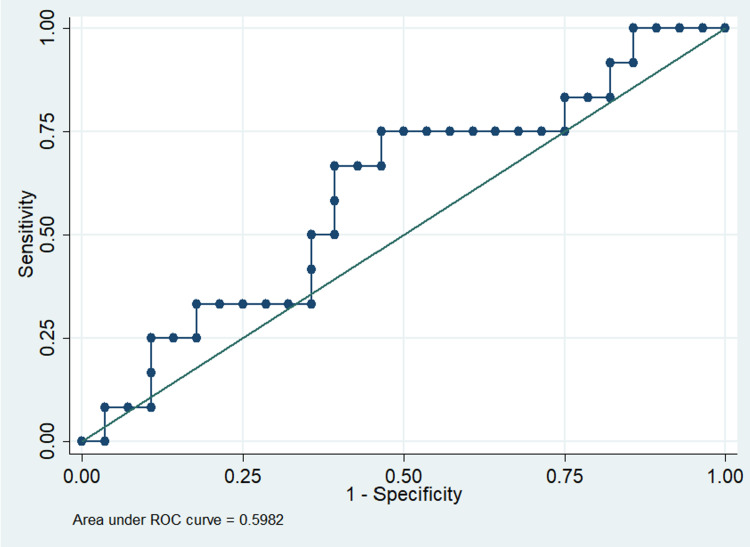
Introduction The passive leg raising (PLR) test is a simple, non-invasive method of knowing fluid responsiveness by acting as an internal-fluid challenge. The PLR test coupled with a non-invasive assessment of stroke volume would be the ideal method to assess fluid responsiveness. This study aimed to determine the correlation between transthoracic echocardiographic cardiac output (TTE-CO) and common carotid artery blood flow (CCABF) parameters in determining fluid responsiveness with the PLR test. Methods We performed a prospective observational study on 40 critically ill patients. Patients were evaluated with a 7-13 MHz linear transducer probe for CCABF parameters calculated using time-averaged mean velocity (TAmean) and with a 1-5 MHz cardiac probe equipped with tissue doppler imaging (TDI) for TTE-CO calculated using left ventricular outflow tract velocity time integral (LVOT VTI) with an apical five-chamber view. Two separate PLR tests (five minutes apart) were done within 48 hours of ICU admission. The first PLR test was to assess the effects on TTE-CO. The second PLR test was performed to assess the effects on CCABF parameters. Patients were designated as fluid responders (FR) if changes in TTE-CO (Δ TTE-CO) ≥ 10 %. Results A positive PLR test was observed in 33% of patients. A strong correlation was present between absolute values of TTE-CO calculated using LVOT VTI and the absolute values of CCABF calculated using TAmean (r=0.60, p<0.05). However, a weak correlation was found between Δ TTE-CO and changes in CCABF (Δ CCABF) during the PLR test (r=0.05, p<0.74). A positive PLR test response could not be detected by Δ CCABF (area under the curve (AUC): 0.59 ± 0.09). Conclusions We found a moderate correlation between TTE-CO and CCABF at baseline. However, Δ TTE-CO had a very poor correlation with Δ CCABF, during the PLR test. Considering this, CCABF parameters may not be recommended as a means to detect fluid responsiveness with PLR tests in critically ill patients.
Keywords: carotid doppler; fluid responsiveness; lvot vti; passive leg raising test; transthoracic echocardiography.
Copyright © 2023, Patnaik et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures








Similar articles
-
Can bioimpedance cardiography assess hemodynamic response to passive leg raising in critically ill patients: A STROBE-compliant study.Medicine (Baltimore). 2020 Dec 18;99(51):e23764. doi: 10.1097/MD.0000000000023764. Medicine (Baltimore). 2020. PMID: 33371141 Free PMC article.
-
Passive leg raising test using the carotid flow velocity-time integral to predict fluid responsiveness.J Ultrasound. 2024 Mar;27(1):97-104. doi: 10.1007/s40477-023-00824-1. Epub 2023 Sep 5. J Ultrasound. 2024. PMID: 37668901 Free PMC article.
-
[The value of passive leg raising test in predicting fluid responsiveness in patients with sepsis-induced cardiac dysfunction].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2015 Sep;27(9):729-34. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2015. PMID: 26955698 Chinese.
-
Rationale for using the velocity-time integral and the minute distance for assessing the stroke volume and cardiac output in point-of-care settings.Ultrasound J. 2020 Apr 21;12(1):21. doi: 10.1186/s13089-020-00170-x. Ultrasound J. 2020. PMID: 32318842 Free PMC article. Review.
-
Predictors of fluid responsiveness in critically ill patients mechanically ventilated at low tidal volumes: systematic review and meta-analysis.Ann Intensive Care. 2021 Feb 8;11(1):28. doi: 10.1186/s13613-021-00817-5. Ann Intensive Care. 2021. PMID: 33555488 Free PMC article. Review.
Cited by
-
Agreement between carotid and LVOT non-invasive cardiac output measurements in ED septic shock patients: a prospective observational study.Sci Rep. 2025 Jun 6;15(1):19911. doi: 10.1038/s41598-025-05077-y. Sci Rep. 2025. PMID: 40481087 Free PMC article.
-
The left ventricular outflow tract and carotid artery velocity time integrals.Front Med Technol. 2024 Jan 24;6:1320810. doi: 10.3389/fmedt.2024.1320810. eCollection 2024. Front Med Technol. 2024. PMID: 38333734 Free PMC article.
References
-
- Fluid resuscitation in septic shock: a positive fluid balance and elevated central venous pressure are associated with increased mortality. Boyd JH, Forbes J, Nakada TA, Walley KR, Russell JA. Crit Care Med. 2011;39:259–265. - PubMed
-
- Passive leg raising predicts fluid responsiveness in the critically ill. Monnet X, Rienzo M, Osman D, Anguel N, Richard C, Pinsky MR, Teboul JL. Crit Care Med. 2006;34:1402–1407. - PubMed
-
- Monnet X, Teboul JL. Applied Physiology in Intensive Care Medicine 2: Physiological Reviews and Editorials. Berlin: Springer-Verlag; 2012. Passive leg raising; pp. 55–59.
-
- Dynamic changes in arterial waveform derived variables and fluid responsiveness in mechanically ventilated patients: a systematic review of the literature. Marik PE, Cavallazzi R, Vasu T, Hirani A. Crit Care Med. 2009;37:2642–2647. - PubMed
-
- Intravascular volume monitoring and extravascular lung water in septic patients with pulmonary edema. Boussat S, Jacques T, Levy B, Laurent E, Gache A, Capellier G, Neidhardt A. Intensive Care Med. 2002;28:712–718. - PubMed
LinkOut - more resources
Full Text Sources