

Transforaminal endoscopic thoracic discectomy: surgical technique
- PMID: 37435321
- PMCID: PMC10331499
- DOI: 10.21037/jss-22-109
Transforaminal endoscopic thoracic discectomy: surgical technique
Abstract
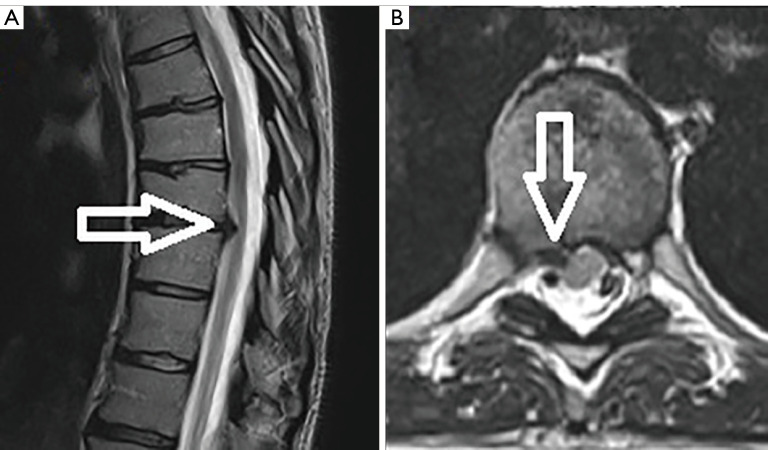
The major challenge inherent to the surgical treatment of thoracic disc herniations is that the disc herniation is often ventral to the spinal cord. Posterior approaches are difficult and dangerous due to the morbidity associated with retraction of the thoracic spinal cord. A ventral approach is not feasible due to the thoracic viscera. A lateral transcavitary approach is the standard for treating ventral thoracic disc pathology but is also quite morbid. Transforaminal endoscopic spine surgery has emerged as a minimally invasive technique for treating thoracic disc pathology and it can be performed in the outpatient setting even with the patient awake. Advances in endoscopic camera technologies as well as the availability of specialty instruments that can be used down a working channel endoscope has now made a myriad of spine pathologies accessible to the minimally invasive spine surgeon. The transforaminal approach and the angled endoscopic camera are an ideal combination for creating a technical advantage to accessing thoracic disc pathology in a minimally invasive fashion. The principal challenges to the approach are needle targeting and understanding the endoscopic visual anatomy. Many surgeons interested in pursuing this technique are often deterred by the burden of the cost and time it takes to become adept and performing the technique. Detailed here are the authors' step-by-step technique and illustrative video that demonstrate transforaminal endoscopic thoracic discectomy (TETD).
Keywords: Endoscopic discectomy; minimally invasive; thoracic disc; transforaminal.
2023 Journal of Spine Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: Both authors have completed the ICMJE uniform disclosure form (available at https://jss.amegroups.com/article/view/10.21037/jss-22-109/coif). AET serves as an unpaid editorial board member of Journal of Spine Surgery from December 2022 to November 2024. The other author has no conflicts of interest to declare.
Figures






Comment in
-
Expanding indications of full endoscopic spine surgery.J Spine Surg. 2023 Sep 22;9(3):229-232. doi: 10.21037/jss-23-65. Epub 2023 Jun 27. J Spine Surg. 2023. PMID: 37841778 Free PMC article. No abstract available.
-
Full-endoscopic thoracic spine approaches.J Spine Surg. 2023 Sep 22;9(3):238-241. doi: 10.21037/jss-23-73. Epub 2023 Jul 20. J Spine Surg. 2023. PMID: 37841798 Free PMC article. No abstract available.
References
LinkOut - more resources
Full Text Sources