

The importance of Hounsfield units in adult spinal deformity surgery: finding an optimal threshold to minimize the risk of mechanical complications
- PMID: 37435329
- PMCID: PMC10331500
- DOI: 10.21037/jss-22-102
The importance of Hounsfield units in adult spinal deformity surgery: finding an optimal threshold to minimize the risk of mechanical complications
Abstract
Background: Low bone mineral density (BMD) is a well-established risk factor for mechanical complications following adult spinal deformity (ASD) surgery. Hounsfield units (HU) measured on computed tomography (CT) scans are a proxy of BMD. In ASD surgery, we sought to: (I) evaluate the association of HU with mechanical complications and reoperation, and (II) identify optimal HU threshold to predict the occurrence of mechanical complications.
Methods: A single-institution retrospective cohort study was undertaken for patients undergoing ASD surgery from 2013-2017. Inclusion criteria were: ≥5-level fusion, sagittal/coronal deformity, and 2-year follow-up. HU were measured on 3 axial slices of one vertebra, either at the upper instrumented vertebra (UIV) itself or UIV ±4 from CT scans. Multivariable regression controlled for age, body mass index (BMI), postoperative sagittal vertical axis (SVA), and postoperative pelvic-incidence lumbar-lordosis mismatch.
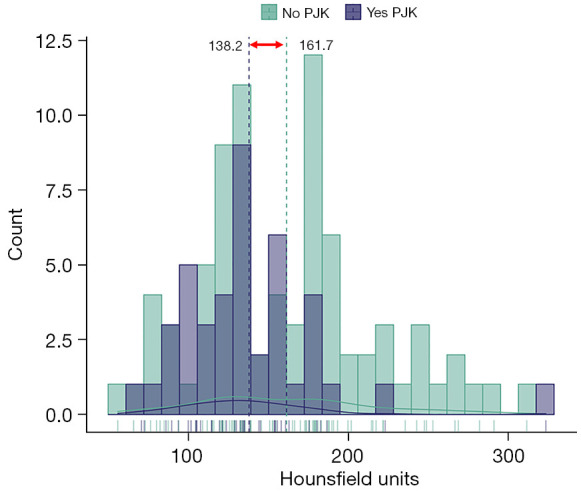
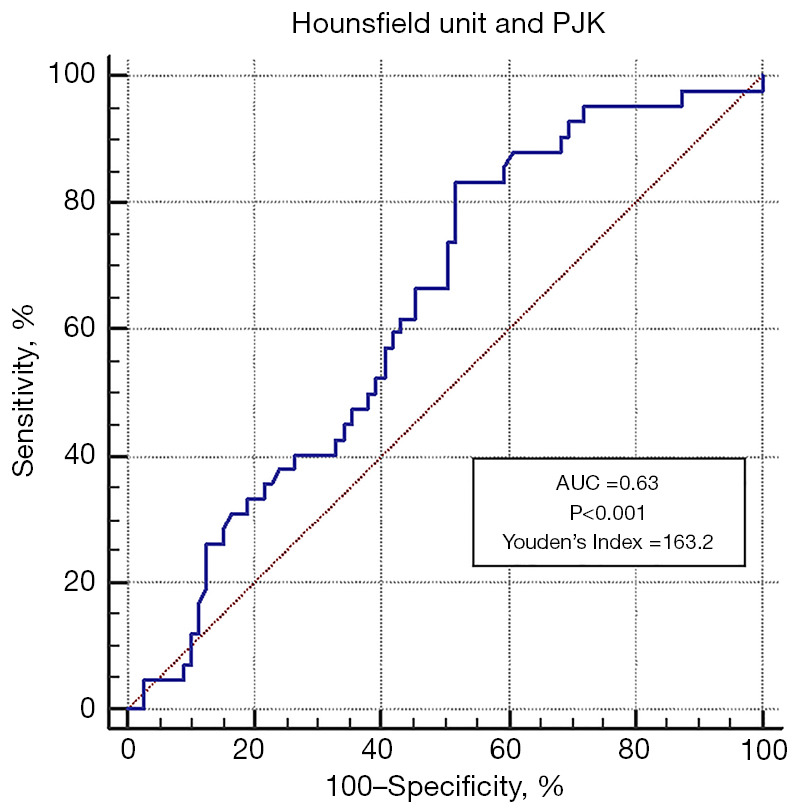
Results: Of 145 patients undergoing ASD surgery, 121 (83.4%) had a preoperative CT from which HU were measured. Mean age was 64.4±10.7 years, mean total instrumented levels was 9.8±2.6, and mean HU was 153.5±52.8. Mean preoperative SVA and T1PA were 95.5±71.1 mm and 28.8°±12.8°, respectively. Postoperative SVA and T1PA significantly improved to 61.2±61.6 mm (P<0.001) and 23.0°±11.0° (P<0.001). Mechanical complications occurred in 74 (61.2%) patients, including 42 (34.7%) proximal junctional kyphosis (PJK), 3 (2.5%) distal junctional kyphosis (DJK), 9 (7.4%) implant failure, 48 (39.7%) rod fracture/pseudarthrosis, and 61 (52.2%) reoperations within 2 years. Univariate logistic regression showed a significant association between low HU and PJK [odds ratio (OR) =0.99; 95% confidence interval (CI): 0.98-0.99; P=0.023], but not on multivariable analysis. No association was found regarding other mechanical complications, overall reoperations, and reoperations due to PJK. HU below 163 were associated with increased PJK on receiver operating characteristic (ROC) curve analysis [area under the curve (AUC) =0.63; 95% CI: 0.53-0.73; P<0.001].
Conclusions: Though several factors contribute to PJK, it appears that 163 HU may serve as a preliminary threshold when planning ASD surgery to mitigate the risk of PJK.
Keywords: Adult spinal deformity (ASD); Hounsfield unit; mechanical complications; proximal junctional kyphosis (PJK); reoperations.
2023 Journal of Spine Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jss.amegroups.com/article/view/10.21037/jss-22-102/coif). SLZ serves as an unpaid editorial board member of Journal of Spine Surgery. SLZ reports being an unaffiliated neurotrauma consultant for the National Football League. BFS is a consultant for Nuvasive and Carbofix and receives institutional research support from Nuvasive and Stryker Spine. AMA received an institutional research support from Stryker Spine. The other authors have no conflicts of interest to declare.
Figures

Similar articles
-
The association between lower Hounsfield units of the upper instrumented vertebra and proximal junctional kyphosis in adult spinal deformity surgery with a minimum 2-year follow-up.Neurosurg Focus. 2020 Aug;49(2):E7. doi: 10.3171/2020.5.FOCUS20192. Neurosurg Focus. 2020. PMID: 32738804
-
Which Bone Mineral Density Measure Offers a More Reliable Prediction of Mechanical Complications in Adult Spinal Deformity Surgery: Hounsfield Units or DEXA Scan?World Neurosurg. 2023 Oct;178:e657-e665. doi: 10.1016/j.wneu.2023.07.140. Epub 2023 Aug 4. World Neurosurg. 2023. PMID: 37543204
-
The Relationship between the Hounsfield Units Value of the Upper Instrumented Vertebra and the Severity of Proximal Junctional Fracture after Adult Spinal Deformity Surgery.Medicina (Kaunas). 2023 Jun 4;59(6):1086. doi: 10.3390/medicina59061086. Medicina (Kaunas). 2023. PMID: 37374290 Free PMC article.
-
The association between bone mineral density and proximal junctional kyphosis in adult spinal deformity: a systematic review and meta-analysis.J Neurosurg Spine. 2023 Apr 7;39(1):82-91. doi: 10.3171/2023.2.SPINE221101. Print 2023 Jul 1. J Neurosurg Spine. 2023. PMID: 37029673
-
Characteristics and risk factors for proximal junctional kyphosis in adult spinal deformity after correction surgery: a systematic review and meta-analysis.Neurosurg Rev. 2019 Sep;42(3):671-682. doi: 10.1007/s10143-018-1004-7. Epub 2018 Jul 7. Neurosurg Rev. 2019. PMID: 29982856
Cited by
-
Opportunistic Osteoporosis Assessment and Fracture Risk Determination Using Cancellous Density Measurement in Hounsfield Units of Native Lumbar Computed Tomography Images-A Comparative Study with Conventional Bone Density Evaluation.J Clin Med. 2025 Feb 13;14(4):1226. doi: 10.3390/jcm14041226. J Clin Med. 2025. PMID: 40004756 Free PMC article.
-
Surgical Management of Adult Spinal Deformity Patients with Osteoporosis.J Clin Med. 2024 Nov 26;13(23):7173. doi: 10.3390/jcm13237173. J Clin Med. 2024. PMID: 39685632 Free PMC article. Review.
-
Does Baseline Hounsfield Unit Predict Patients' Outcomes Following Surgical Management of Unstable Osteoporotic Thoracolumbar Fractures?Medicina (Kaunas). 2025 Jan 27;61(2):227. doi: 10.3390/medicina61020227. Medicina (Kaunas). 2025. PMID: 40005344 Free PMC article.
-
Hounsfield units and vertebral bone quality score for predicting mechanical complications after adult spinal deformity surgery: a systematic review and meta-analysis.Asian Spine J. 2024 Oct;18(5):719-730. doi: 10.31616/asj.2023.0402. Epub 2024 Oct 22. Asian Spine J. 2024. PMID: 39434231 Free PMC article.
-
The Association Between Hounsfield Units and Mechanical Failure in ASD Patients.Global Spine J. 2025 May;15(4):2218-2225. doi: 10.1177/21925682241291519. Epub 2024 Oct 13. Global Spine J. 2025. PMID: 39397242 Free PMC article.
References
-
- Schwab F, Dubey A, Gamez L, et al. Adult scoliosis: prevalence, SF-36, and nutritional parameters in an elderly volunteer population. Spine (Phila Pa 1976) 2005;30:1082-5. 10.1097/01.brs.0000160842.43482.cd - DOI - PubMed
LinkOut - more resources
Full Text Sources