

A tablet-based quantitative assessment of manual dexterity for detection of early psychosis
- PMID: 37435404
- PMCID: PMC10330763
- DOI: 10.3389/fpsyt.2023.1200864
A tablet-based quantitative assessment of manual dexterity for detection of early psychosis
Abstract
Background: We performed a pilot study on whether tablet-based measures of manual dexterity can provide behavioral markers for detection of first-episode psychosis (FEP), and whether cortical excitability/inhibition was altered in FEP.
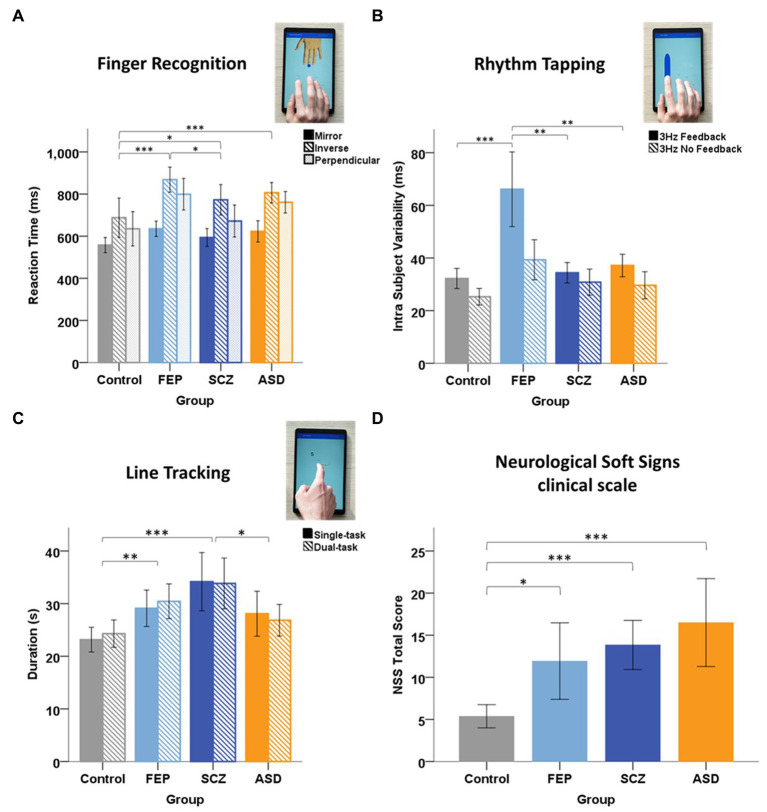
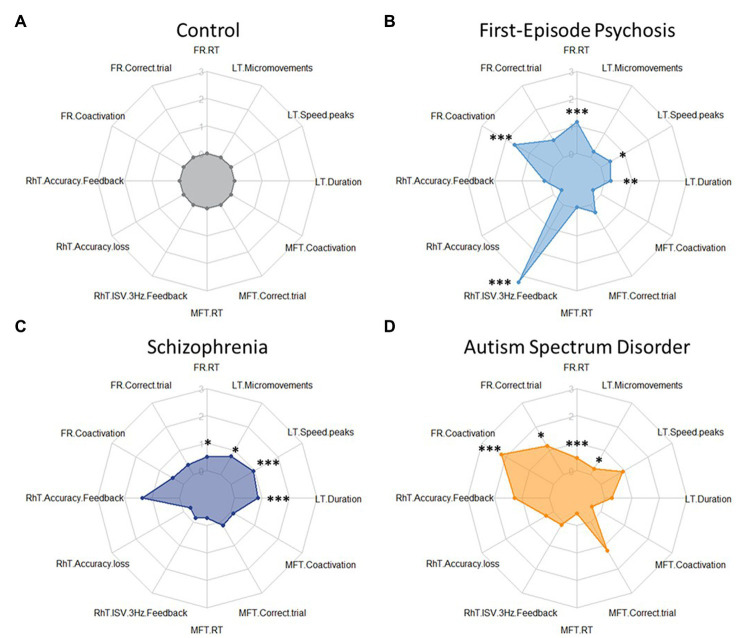
Methods: Behavioral and neurophysiological testing was undertaken in persons diagnosed with FEP (N = 20), schizophrenia (SCZ, N = 20), autism spectrum disorder (ASD, N = 20), and in healthy control subjects (N = 20). Five tablet tasks assessed different motor and cognitive functions: Finger Recognition for effector (finger) selection and mental rotation, Rhythm Tapping for temporal control, Sequence Tapping for control/memorization of motor sequences, Multi Finger Tapping for finger individuation, and Line Tracking for visuomotor control. Discrimination of FEP (from other groups) based on tablet-based measures was compared to discrimination through clinical neurological soft signs (NSS). Cortical excitability/inhibition, and cerebellar brain inhibition were assessed with transcranial magnetic stimulation.
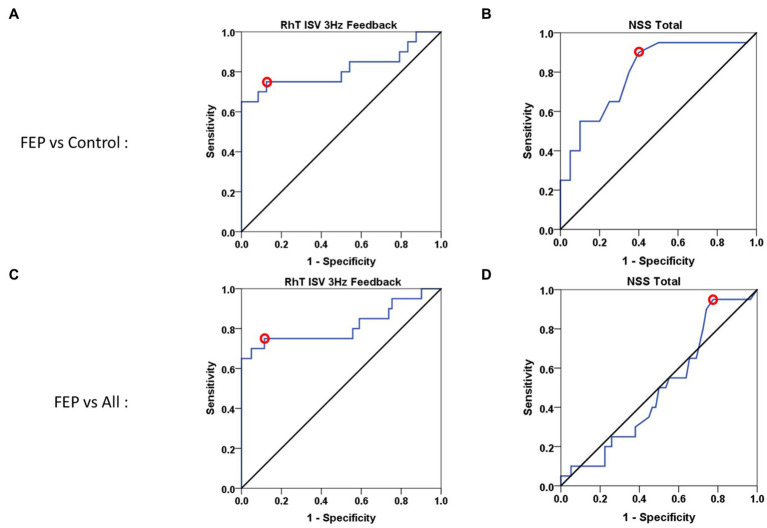
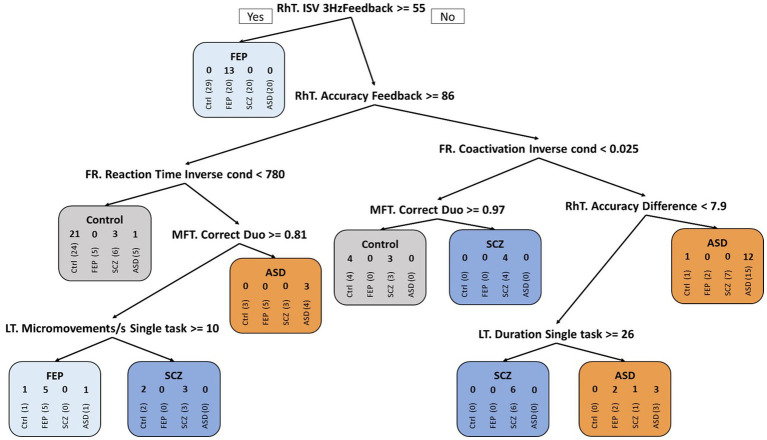
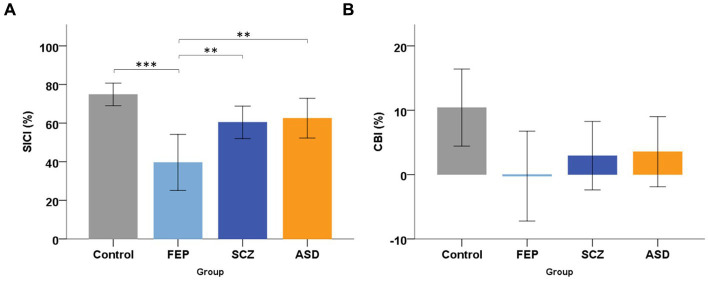
Results: Compared to controls, FEP patients showed slower reaction times and higher errors in Finger Recognition, and more variability in Rhythm Tapping. Variability in Rhythm Tapping showed highest specificity for the identification of FEP patients compared to all other groups (FEP vs. ASD/SCZ/Controls; 75% sensitivity, 90% specificity, AUC = 0.83) compared to clinical NSS (95% sensitivity, 22% specificity, AUC = 0.49). Random Forest analysis confirmed FEP discrimination vs. other groups based on dexterity variables (100% sensitivity, 85% specificity, balanced accuracy = 92%). The FEP group had reduced short-latency intra-cortical inhibition (but similar excitability) compared to controls, SCZ, and ASD. Cerebellar inhibition showed a non-significant tendency to be weaker in FEP.
Conclusion: FEP patients show a distinctive pattern of dexterity impairments and weaker cortical inhibition. Easy-to-use tablet-based measures of manual dexterity capture neurological deficits in FEP and are promising markers for detection of FEP in clinical practice.
Keywords: Transcranial Magnetic Stimulation (TMS); autism spectrum disorder (ASD); behavioral marker; first-episode psychosis (FEP); manual dexterity; schizophrenia; tablet-based assessment.
Copyright © 2023 Le Boterff, Rabah, Carment, Bendjemaa, Térémetz, Alouit, Levy, Tanguy, Morin, Amado, Cuenca, Turc, Maier, Krebs and Lindberg.
Conflict of interest statement
MT and PL own shares in Dextrain company (www.dextrain.com) which develops and commercializes solutions for measurement and rehabilitation of manual dexterity. MT, MM, and PL have a patent on the DexTrain manipulandum (WO2020070305A1) and method for evaluating manual dexterity (WO2016184935A2). The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
A novel tablet-based application for assessment of manual dexterity and its components: a reliability and validity study in healthy subjects.J Neuroeng Rehabil. 2022 Mar 24;19(1):35. doi: 10.1186/s12984-022-01011-9. J Neuroeng Rehabil. 2022. PMID: 35331273 Free PMC article.
-
Manual Dexterity in Schizophrenia-A Neglected Clinical Marker?Front Psychiatry. 2017 Jul 10;8:120. doi: 10.3389/fpsyt.2017.00120. eCollection 2017. Front Psychiatry. 2017. PMID: 28740470 Free PMC article.
-
Manual Dexterity and Aging: A Pilot Study Disentangling Sensorimotor From Cognitive Decline.Front Neurol. 2018 Oct 29;9:910. doi: 10.3389/fneur.2018.00910. eCollection 2018. Front Neurol. 2018. PMID: 30420830 Free PMC article.
-
[Sensorimotor aspects and manual dexterity in autism spectrum disorders: A literature review].Encephale. 2020 Apr;46(2):135-145. doi: 10.1016/j.encep.2019.11.005. Epub 2020 Jan 9. Encephale. 2020. PMID: 31928741 Review. French.
-
Deficits in social cognition in first episode psychosis: A review of the literature.Clin Psychol Rev. 2016 Dec;50:108-137. doi: 10.1016/j.cpr.2016.10.001. Epub 2016 Oct 11. Clin Psychol Rev. 2016. PMID: 27771557 Review.
Cited by
-
Functional upper-extremity movements in autism: A narrative literature review.Res Autism Spectr Disord. 2024 Oct;118:102489. doi: 10.1016/j.rasd.2024.102489. Epub 2024 Oct 10. Res Autism Spectr Disord. 2024. PMID: 40821657
-
Neurophysiological explorations across the spectrum of psychosis, autism, and depression, during wakefulness and sleep: protocol of a prospective case-control transdiagnostic multimodal study (DEMETER).BMC Psychiatry. 2023 Nov 21;23(1):860. doi: 10.1186/s12888-023-05347-x. BMC Psychiatry. 2023. PMID: 37990173 Free PMC article.
References
LinkOut - more resources
Full Text Sources