

Linsitinib, an IGF-1R inhibitor, attenuates disease development and progression in a model of thyroid eye disease
- PMID: 37435490
- PMCID: PMC10331459
- DOI: 10.3389/fendo.2023.1211473
Linsitinib, an IGF-1R inhibitor, attenuates disease development and progression in a model of thyroid eye disease
Abstract
Introduction: Graves' disease (GD) is an autoimmune disorder caused by autoantibodies against the thyroid stimulating hormone receptor (TSHR) leading to overstimulation of the thyroid gland. Thyroid eye disease (TED) is the most common extra thyroidal manifestation of GD. Therapeutic options to treat TED are very limited and novel treatments need to be developed. In the present study we investigated the effect of linsitinib, a dual small-molecule kinase inhibitor of the insulin-like growth factor 1 receptor (IGF-1R) and the Insulin receptor (IR) on the disease outcome of GD and TED.
Methods: Linsitinib was administered orally for four weeks with therapy initiating in either the early ("active") or the late ("chronic") phases of the disease. In the thyroid and the orbit, autoimmune hyperthyroidism and orbitopathy were analyzed serologically (total anti-TSHR binding antibodies, stimulating anti TSHR antibodies, total T4 levels), immunohistochemically (H&E-, CD3-, TNFa- and Sirius red staining) and with immunofluorescence (F4/80 staining). An MRI was performed to quantify in vivo tissue remodeling inside the orbit.
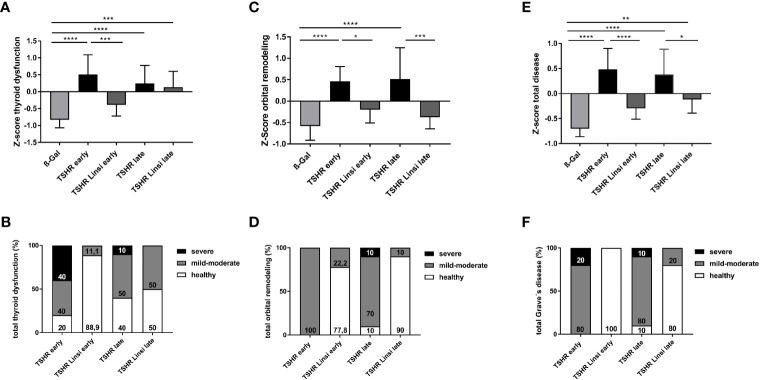
Results: Linsitinib prevented autoimmune hyperthyroidism in the early state of the disease, by reducing morphological changes indicative for hyperthyroidism and blocking T-cell infiltration, visualized by CD3 staining. In the late state of the disease linsitinib had its main effect in the orbit. Linsitinib reduced immune infiltration of T-cells (CD3 staining) and macrophages (F4/80 and TNFa staining) in the orbita in experimental GD suggesting an additional, direct effect of linsitinib on the autoimmune response. In addition, treatment with linsitinib normalized the amount of brown adipose tissue in both the early and late group. An in vivo MRI of the late group was performed and revealed a marked decrease of inflammation, visualized by 19F MR imaging, significant reduction of existing muscle edema and formation of brown adipose tissue.
Conclusion: Here, we demonstrate that linsitinib effectively prevents development and progression of thyroid eye disease in an experimental murine model for Graves' disease. Linsitinib improved the total disease outcome, indicating the clinical significance of the findings and providing a path to therapeutic intervention of Graves' Disease. Our data support the use of linsitinib as a novel treatment for thyroid eye disease.
Keywords: Graves’ disease (GD); IGF-1R; autoimmune disorder; inflammation; linsitinib; thyroid eye disease (TED).
Copyright © 2023 Gulbins, Horstmann, Daser, Flögel, Oeverhaus, Bechrakis, Banga, Keitsch, Wilker, Krause, Hammer, Spencer, Zeidan, Eckstein, Philipp and Görtz.
Conflict of interest statement
Authors AS and RZ were employed by the company Sling Therapeutics Inc. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures








References
-
- Pritchard J, Han R, Horst N, Cruikshank WW, Smith. Immunoglobulin activation of T cell chemoattractant expression in fibroblasts from patients with graves’ disease is mediated through the insulin-like growth factor I receptor pathway. J Immunol (2003) 170(12):6348–54. doi: 10.4049/jimmunol.170.12.6348 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources