

Antibody-drug conjugates: the evolving field of targeted chemotherapy for breast cancer treatment
- PMID: 37435563
- PMCID: PMC10331351
- DOI: 10.1177/17588359231183679
Antibody-drug conjugates: the evolving field of targeted chemotherapy for breast cancer treatment
Abstract
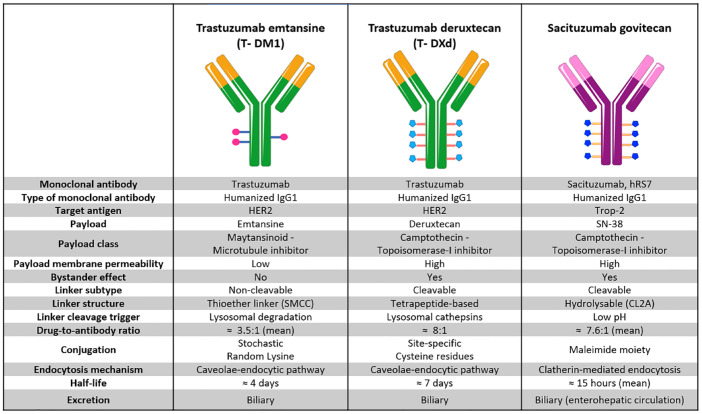
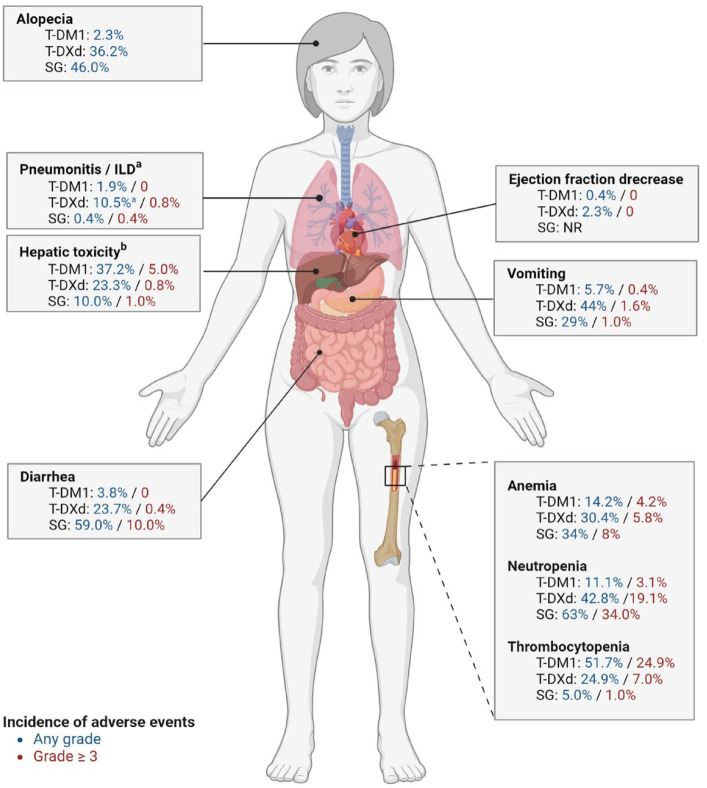
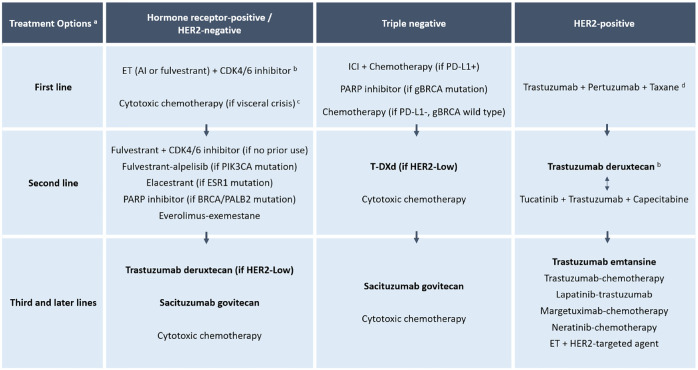
Antibody-drug conjugates (ADCs) are a class of antineoplastic agents whose structure is composed of three main components: a monoclonal antibody (mAB) targeting a specific target antigen, a cytotoxic payload, and a linker binding the antibody to the payload. By combining the specificity of mABs with the high potency of the payloads, ADCs constitute a smart drug delivery system with improved therapeutic index. After recognition and binding of the mAB to its target surface antigen, ADCs are internalized by endocytosis by the tumor cell, releasing the payloads into the cytoplasm, where they exert their cytotoxic activity, eventually leading to cell death. The composition of some of the new ADCs confers additional functional properties that allow expanding their activity to neighboring cells not expressing the target antigen, constituting a valuable strategy to overcome tumor heterogeneity. Some of these 'off-target effects', such as the bystander effect, are possibly the mechanism underlying the antitumor activity demonstrated in patients with low expression of the target antigens, which represents an important paradigm shift in anticancer targeted therapy. Three ADCs are currently approved for the treatment of breast cancer (BC); two anti-HER2 (human epidermal growth factor receptor 2) ADCs (trastuzumab emtansine and trastuzumab deruxtecan); and one Trop-2-targeted ADC (sacituzumab govitecan). Based on the unprecedented efficacy data demonstrated by these agents, ADCs have been incorporated as part of standard regimens for all subtypes of advanced BC, as well as for high-risk early HER2-positive BC. Despite the remarkable advances, several hurdles still remain to overcome, including the development of reliable biomarkers for patient selection, prevention, and management of potentially severe toxicities, ADC resistance mechanisms, post-ADC resistance patterns, and optimal treatment sequencing and combinations. In this review, we will summarize the currently available evidence related to the use of these agents, as well as explore the current landscape of ADC development for BC treatment.
Keywords: antibody–drug conjugates; breast cancer; targeted therapy.
© The Author(s), 2023.
Figures
References
-
- Alnaim L. Therapeutic drug monitoring of cancer chemotherapy. J Oncol Pharm Pract 2007; 13: 207–221. - PubMed
-
- Gerber DE. Targeted therapies: a new generation of cancer treatments. Am Fam Physician GP 2008; 77: 311–319. - PubMed
-
- Inoue K, Nakagami K, Mizutani M, et al. Randomized phase III trial of trastuzumab monotherapy followed by trastuzumab plus docetaxel versus trastuzumab plus docetaxel as first-line therapy in patients with HER2-positive metastatic breast cancer: the JO17360 Trial Group. Breast Cancer Res Treat 2010; 119: 127–136. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
