

Clinical and Radiographic Predictors of Successful Coronary Angiography Through Right Radial Artery Access
- PMID: 37435602
- PMCID: PMC10331560
- DOI: 10.15420/icr.2023.04
Clinical and Radiographic Predictors of Successful Coronary Angiography Through Right Radial Artery Access
Abstract
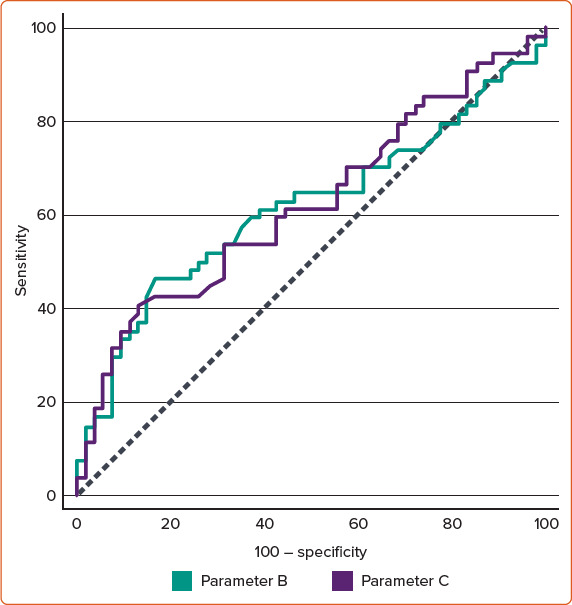
Background: One of the limitations of the right radial access approach is complex vessel anatomy, such as subclavian tortuosity. Several clinical predictors have been proposed for tortuosities, such as older age, female sex and hypertension. In this study, we hypothesised that chest radiography would add predictive value to the traditional predictors. Methods: This prospective blinded study included patients who underwent transradial access coronary angiography. They were classified into four groups according to difficulty: Group I, Group II, Group III and Group IV. Different groups were compared according to clinical and radiographic characteristics. Results: The study included 108 patients (54, 27, 17 and 10 patients in Groups I, II, III and IV, respectively). The rate of crossover to transfemoral access was 9.26%. Age, hypertension and female sex were associated with a greater difficulty and failure rates. Regarding radiographic parameters, a higher failure rate was associated with a higher diameter of the aortic knuckle (Group IV, 4.09 ± 1.32 cm versus Groups I, II and III combined, 3.26 ± 0.98 cm; p=0.015) and the width of the mediastinum (Group IV, 8.96 ± 2.88 cm versus Groups I, II and III combined, 7.28 ± 1.78 cm; p=0.009). The cut-off value for prominent aortic knuckle was 3.55 cm (sensitivity 70% and specificity 67.35%) and the width of mediastinum was 6.59 cm (sensitivity 90% and specificity 42.86%). Conclusion: Radiographic prominent aortic knuckle and wide mediastinum are valuable clinical parameters and useful predictors for transradial access failure caused by tortuosity of the right subclavian/brachiocephalic arteries or aorta.
Keywords: Radial access; coronary angiography; crossover; failure; subclavian tortuosity.
Copyright © 2023, Radcliffe Cardiology.
Conflict of interest statement
Disclosure: The authors have no conflicts of interest to declare. Data availability: The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions. Authors' contributions: Conceptualisation: SE; data curation: SE, AO, MAK; formal analysis: SE, AO, MAK; investigation: SE, AO, MAK; methodology: SE, AO, MAK; project administration: SE; software: SE; supervision: SE; writing – original draft preparation: SE, AO, MAK; writing – review & editing: SE, AO, MAK. Ethics: This study was carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki). Approval was granted by the Ethics Committee of Saudi German Hospital Cairo branch. Consent: Written informed consent was obtained from all individuals included in the study.
Figures



References
-
- Roffi M, Patrono C, Collet JP et al. ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: task force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Am Heart J. 2016;37:267–315. doi: 10.1093/eurheartj/ehv320. - DOI - PubMed
-
- Hamon M, Pristipino C, Di Mario C et al. Consensus document on the radial approach in percutaneous cardiovascular interventions: position paper by the European Association of Percutaneous Cardiovascular Interventions and working groups on acute cardiac care and thrombosis of the European Society of Cardiology. Am Heart J. 2013;8:1242–51. doi: 10.4244/EIJV8I11A192. - DOI - PubMed
LinkOut - more resources
Full Text Sources
