

Electroacupuncture in the treatment of IBS in rats: investigation of the mechanisms of CRH+ neurons in the paraventricular nucleus
- PMID: 37435647
- PMCID: PMC10625839
- DOI: 10.1152/jn.00156.2023
Electroacupuncture in the treatment of IBS in rats: investigation of the mechanisms of CRH+ neurons in the paraventricular nucleus
Abstract
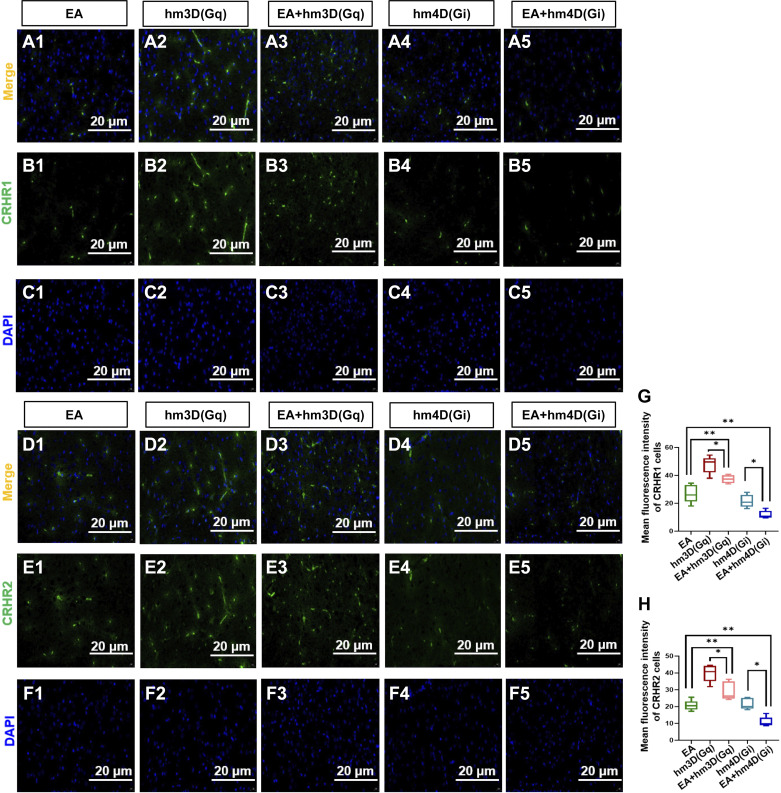
Electroacupuncture (EA) is well documented to treat irritable bowel syndrome (IBS). However, the mechanism of the central nervous system related to IBS and acupuncture stimulation is still not well known. In this study, a rat model of IBS was established by cold-restraint comprehensive stresses for 15 days, and it was found that the levels of corticotropin-releasing hormone (CRH), corticosterone (CORT), and adrenocorticotropic hormone (ACTH) in the peripheral serum were increased; the visceral sensitivity was enhanced; and the intestinal motility was accelerated, specifically, there was an enhancement in the discharge frequency of neurons in the paraventricular nucleus (PVN). EA treatment for 3 days, 20 min/day, alleviated the increase in the levels of CRH, CORT, and ACTH in the peripheral serum of rats, reduced the visceral sensitivity of IBS rats, and inhibited colon movement and discharge frequency of the neurons in the PVN. In addition, EA could reduce the excitability of CRH neurons and the expression of corticotropin-releasing hormone receptor 1 (CRHR1) and corticotropin-releasing hormone receptor 2 (CRHR2) in PVN. At the same time, the expression of CRH, CRHR1, and CRHR2 in the peripheral colon was decreased. Taken together, EA appears to regulate intestinal functional activity through the central CRH nervous system, revealing the central regulation mechanism of EA in IBS rats, and providing a scientific research basis for the correlation among the meridians, viscera, and brain.NEW & NOTEWORTHY The purpose of this research was to determine the central regulatory mechanism of electroacupuncture (EA) in rats with irritable bowel syndrome (IBS). Our results showed that combined with the serum changes in corticotropin-releasing hormone (CRH), corticosterone (CORT), and adrenocorticotropic hormone (ACTH), the improvement of IBS by EA was related to them. Furthermore, EA could regulate intestinal functional activity through the central CRH+ nervous system.
Keywords: corticotropin-releasing hormone; corticotropin-releasing hormone receptor 1; corticotropin-releasing hormone receptor 2; electroacupuncture; irritable bowel syndrome.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures






References
-
- Vandenplas Y, Abkari A, Bellaiche M, Benninga M, Chouraqui JP, Cokura F, Harb T, Hegar B, Lifschitz C, Ludwig T, Miqdady M, de Morais MB, Osatakul S, Salvatore S, Shamir R, Staiano A, Szajewska H, Thapar N. Prevalence and health outcomes of functional gastrointestinal symptoms in infants from birth to 12 months of age. J Pediatr Gastroenterol Nutr 61: 531–537, 2015. [Erratum in J Pediatr Gastroenterol Nutr 62: 516, 2016]. doi:10.1097/MPG.0000000000000949. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources