

Streptococcus Species Abundance in the Gut Is Linked to Subclinical Coronary Atherosclerosis in 8973 Participants From the SCAPIS Cohort
- PMID: 37435755
- PMCID: PMC10399955
- DOI: 10.1161/CIRCULATIONAHA.123.063914
Streptococcus Species Abundance in the Gut Is Linked to Subclinical Coronary Atherosclerosis in 8973 Participants From the SCAPIS Cohort
Abstract
Background: Gut microbiota have been implicated in atherosclerotic disease, but their relation with subclinical coronary atherosclerosis is unclear. This study aimed to identify associations between the gut microbiome and computed tomography-based measures of coronary atherosclerosis and to explore relevant clinical correlates.
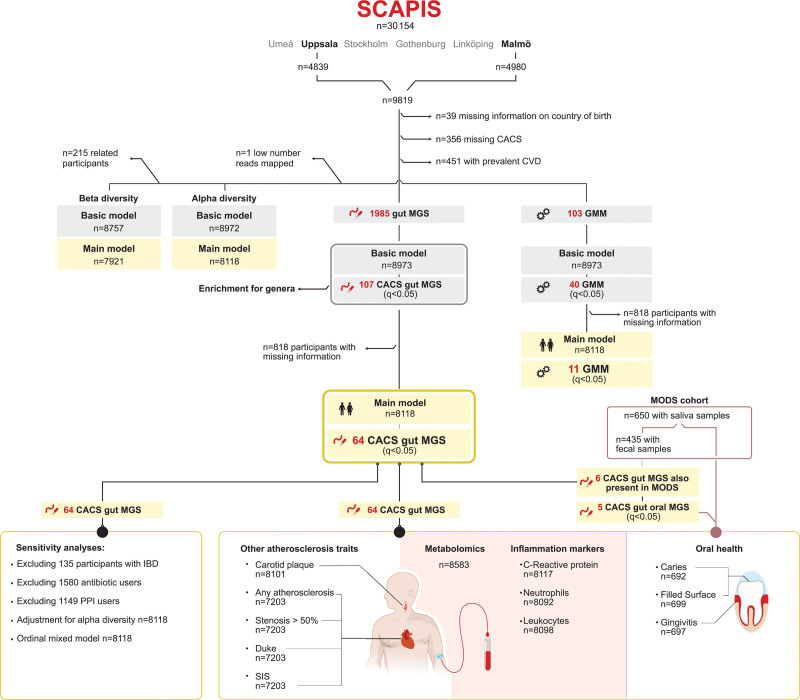
Methods: We conducted a cross-sectional study of 8973 participants (50 to 65 years of age) without overt atherosclerotic disease from the population-based SCAPIS (Swedish Cardiopulmonary Bioimage Study). Coronary atherosclerosis was measured using coronary artery calcium score and coronary computed tomography angiography. Gut microbiota species abundance and functional potential were assessed with shotgun metagenomics sequencing of fecal samples, and associations with coronary atherosclerosis were evaluated with multivariable regression models adjusted for cardiovascular risk factors. Associated species were evaluated for association with inflammatory markers, metabolites, and corresponding species in saliva.
Results: The mean age of the study sample was 57.4 years, and 53.7% were female. Coronary artery calcification was detected in 40.3%, and 5.4% had at least 1 stenosis with >50% occlusion. Sixty-four species were associated with coronary artery calcium score independent of cardiovascular risk factors, with the strongest associations observed for Streptococcus anginosus and Streptococcus oralis subsp oralis (P<1×10-5). Associations were largely similar across coronary computed tomography angiography-based measurements. Out of the 64 species, 19 species, including streptococci and other species commonly found in the oral cavity, were associated with high-sensitivity C-reactive protein plasma concentrations, and 16 with neutrophil counts. Gut microbial species that are commonly found in the oral cavity were negatively associated with plasma indole propionate and positively associated with plasma secondary bile acids and imidazole propionate. Five species, including 3 streptococci, correlated with the same species in saliva and were associated with worse dental health in the Malmö Offspring Dental Study. Microbial functional potential of dissimilatory nitrate reduction, anaerobic fatty acid β-oxidation, and amino acid degradation were associated with coronary artery calcium score.
Conclusions: This study provides evidence of an association of a gut microbiota composition characterized by increased abundance of Streptococcus spp and other species commonly found in the oral cavity with coronary atherosclerosis and systemic inflammation markers. Further longitudinal and experimental studies are warranted to explore the potential implications of a bacterial component in atherogenesis.
Keywords: Streptococcus; atherosclerosis; gastrointestinal microbiome; metagenomics; tomography.
Conflict of interest statement
Figures




Comment in
-
Letter by Li et al Regarding Article, "Streptococcus Species Abundance in the Gut Is Linked to Subclinical Coronary Atherosclerosis in 8973 Participants From the SCAPIS Cohort".Circulation. 2024 Jan 16;149(3):274-275. doi: 10.1161/CIRCULATIONAHA.123.067212. Epub 2024 Jan 16. Circulation. 2024. PMID: 38227716 No abstract available.
References
-
- Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, Barengo NC, Beaton AZ, Benjamin EJ, Benziger CP, et al. ; GBD-NHLBI-JACC Global Burden of Cardiovascular Diseases Writing Group. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76:2982–3021. doi: 10.1016/j.jacc.2020.11.010 - PMC - PubMed
-
- Jonsson AL, Bäckhed F. Role of gut microbiota in atherosclerosis. Nat Rev Cardiol. 2017;14:79–87. doi: 10.1038/nrcardio.2016.183 - PubMed
-
- Chakaroun RM, Olsson LM, Bäckhed F. The potential of tailoring the gut microbiome to prevent and treat cardiometabolic disease. Nat Rev Cardiol. 2023;20:217–235. doi: 10.1038/s41569-022-00771-0 - PubMed
-
- Ott SJ, El Mokhtari NE, Musfeldt M, Hellmig S, Freitag S, Rehman A, Kühbacher T, Nikolaus S, Namsolleck P, Blaut M, et al. Detection of diverse bacterial signatures in atherosclerotic lesions of patients with coronary heart disease. Circulation. 2006;113:929–937. doi: 10.1161/CIRCULATIONAHA.105.579979 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
