

Explainable machine learning model for predicting skeletal muscle loss during surgery and adjuvant chemotherapy in ovarian cancer
- PMID: 37435785
- PMCID: PMC10570082
- DOI: 10.1002/jcsm.13282
Explainable machine learning model for predicting skeletal muscle loss during surgery and adjuvant chemotherapy in ovarian cancer
Abstract
Background: Skeletal muscle loss during treatment is associated with poor survival outcomes in patients with ovarian cancer. Although changes in muscle mass can be assessed on computed tomography (CT) scans, this labour-intensive process can impair its utility in clinical practice. This study aimed to develop a machine learning (ML) model to predict muscle loss based on clinical data and to interpret the ML model by applying SHapley Additive exPlanations (SHAP) method.
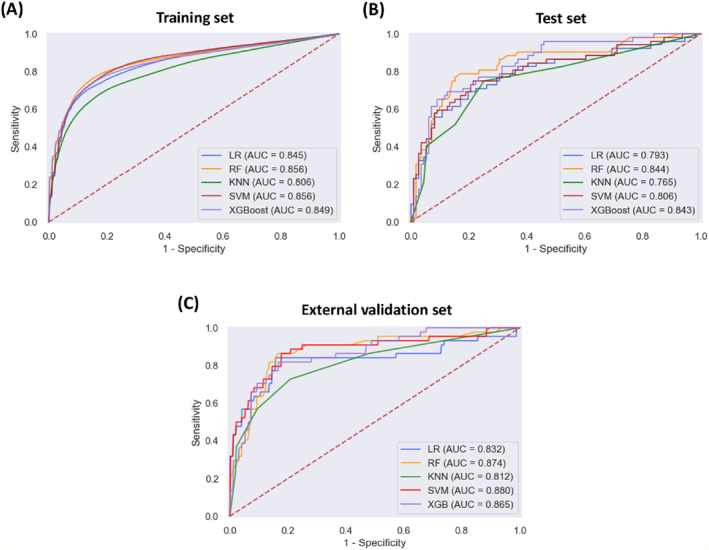
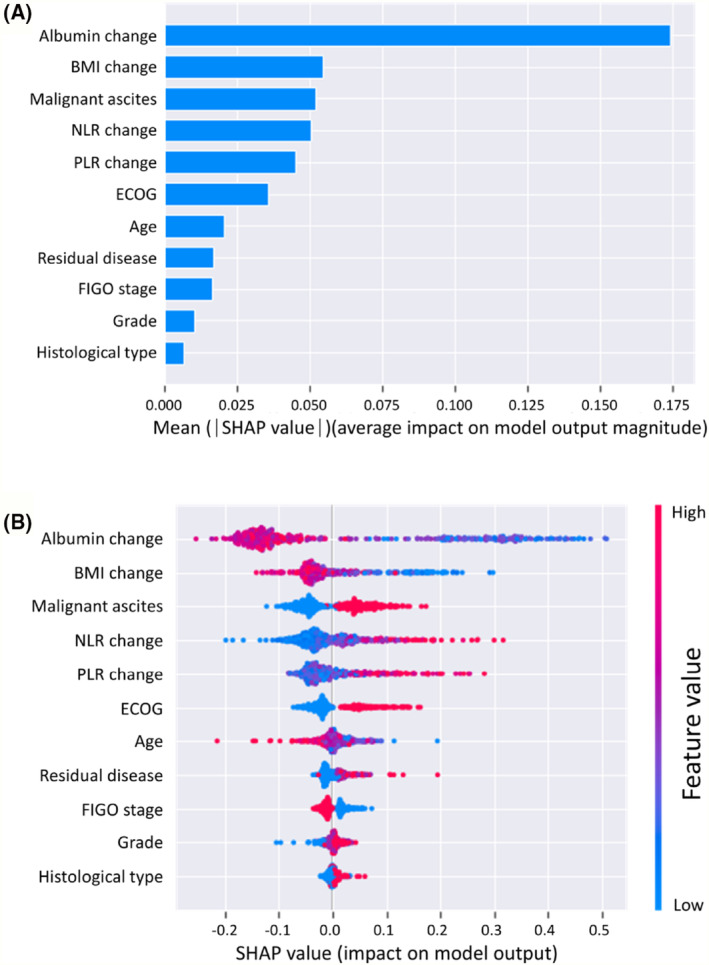
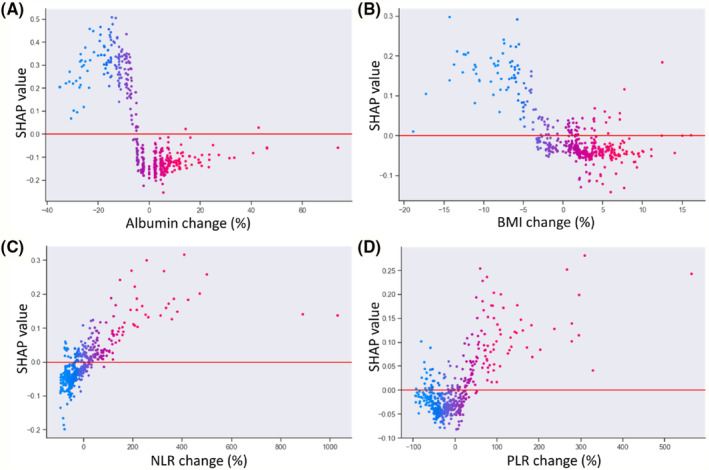
Methods: This study included the data of 617 patients with ovarian cancer who underwent primary debulking surgery and platinum-based chemotherapy at a tertiary centre between 2010 and 2019. The cohort data were split into training and test sets based on the treatment time. External validation was performed using 140 patients from a different tertiary centre. The skeletal muscle index (SMI) was measured from pre- and post-treatment CT scans, and a decrease in SMI ≥ 5% was defined as muscle loss. We evaluated five ML models to predict muscle loss, and their performance was determined using the area under the receiver operating characteristic curve (AUC) and F1 score. The features for analysis included demographic and disease-specific characteristics and relative changes in body mass index (BMI), albumin, neutrophil-to-lymphocyte ratio (NLR), and platelet-to-lymphocyte ratio (PLR). The SHAP method was applied to determine the importance of the features and interpret the ML models.
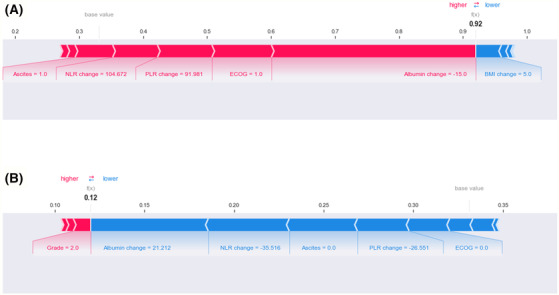
Results: The median (inter-quartile range) age of the cohort was 52 (46-59) years. After treatment, 204 patients (33.1%) experienced muscle loss in the training and test datasets, while 44 (31.4%) patients experienced muscle loss in the external validation dataset. Among the five evaluated ML models, the random forest model achieved the highest AUC (0.856, 95% confidence interval: 0.854-0.859) and F1 score (0.726, 95% confidence interval: 0.722-0.730). In the external validation, the random forest model outperformed all ML models with an AUC of 0.874 and an F1 score of 0.741. The results of the SHAP method showed that the albumin change, BMI change, malignant ascites, NLR change, and PLR change were the most important factors in muscle loss. At the patient level, SHAP force plots demonstrated insightful interpretation of our random forest model to predict muscle loss.
Conclusions: Explainable ML model was developed using clinical data to identify patients experiencing muscle loss after treatment and provide information of feature contribution. Using the SHAP method, clinicians may better understand the contributors to muscle loss and target interventions to counteract muscle loss.
Keywords: SHapley Additive exPlanations; machine learning; muscle loss; ovarian cancer.
© 2023 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by John Wiley & Sons Ltd on behalf of Society on Sarcopenia, Cachexia and Wasting Disorders.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71:209–249. - PubMed
-
- McSharry V, Glennon K, Mullee A, Brennan D. The impact of body composition on treatment in ovarian cancer: a current insight. Expert Rev Clin Pharmacol 2021;14:1065–1074. - PubMed
-
- Polen‐de C, Fadadu P, Weaver AL, Moynagh M, Takahashi N, Jatoi A, et al. Quality is more important than quantity: pre‐operative sarcopenia is associated with poor survival in advanced ovarian cancer. Int J Gynecol Cancer 2022;32:1289–1296. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
