

Symptoms associated with headache in youth
- PMID: 37435790
- PMCID: PMC10852031
- DOI: 10.1177/03331024231187162
Symptoms associated with headache in youth
Abstract
Objective: To determine the underlying relationships between a broad range of headache-associated symptoms and how they relate to headache burden.
Background: Symptoms associated with head pain inform classification of headache disorders. However, many headache-associated symptoms are not included in the diagnostic criteria, which is largely based on expert opinion. Large symptom databases can assess headache-associated symptoms irrespective of pre-existing diagnostic categories.
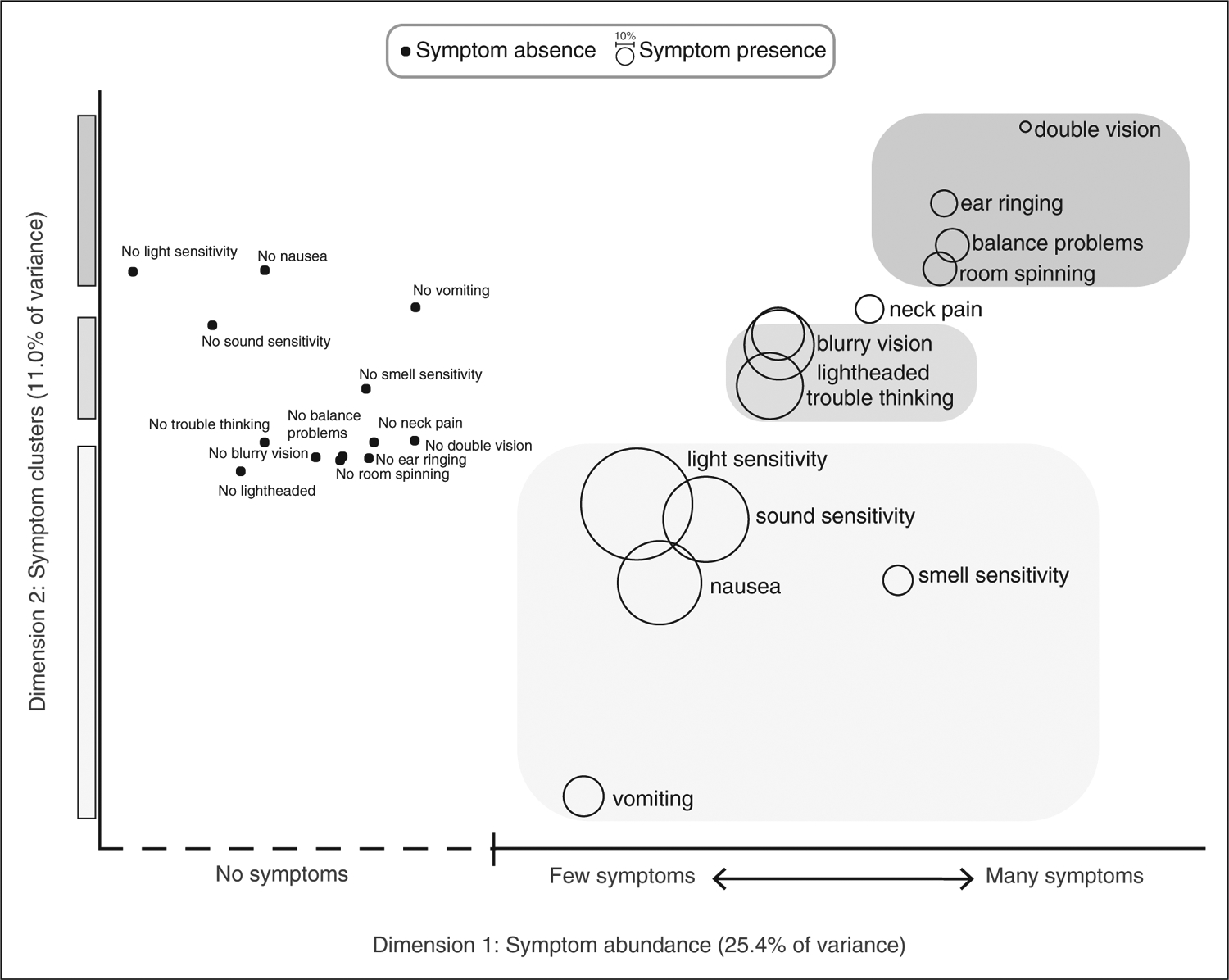
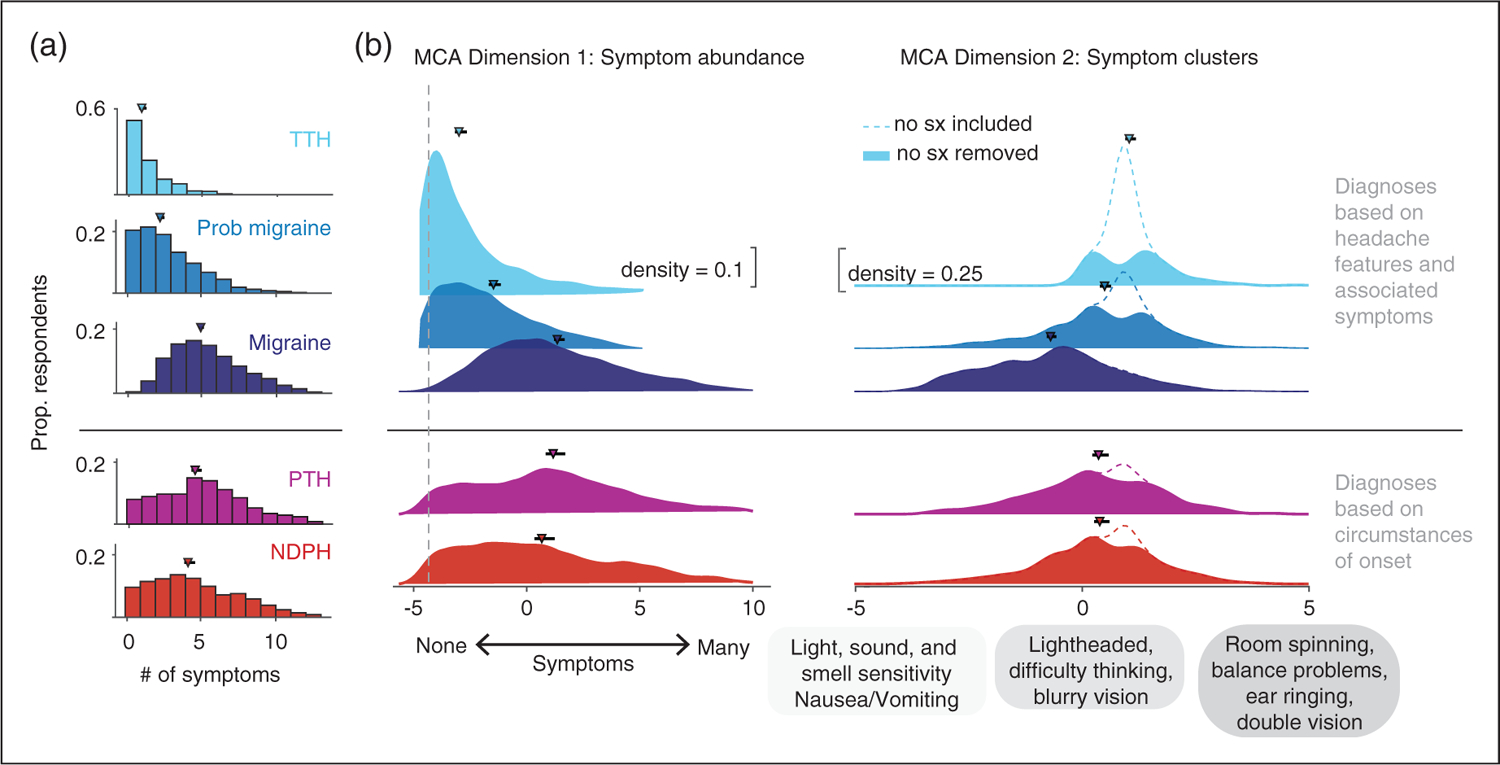
Methods: We conducted a large single-center cross-sectional study on youth (6-17 years old) assessing patient-reported outpatient headache questionnaires between June 2017 and February 2022. Multiple correspondence analysis, an exploratory factor analysis, was applied to 13 headache-associated symptoms.
Results: 6662 participants (64% female; median age 13.6 years) were included. Multiple correspondence analysis dimension 1 (25.4% of the variance) captured the absence or abundance of headache-associated symptoms. A greater number of headache-associated symptoms correlated with greater headache burden. Dimension 2 (11.0% of the variance) revealed three symptom clusters: (1) cardinal features of migraine (light, sound, and smell sensitivity, nausea, and vomiting), (2) nonspecific global neurologic dysfunction symptoms (lightheadedness, trouble thinking, blurry vision), (3) vestibular and brainstem dysfunction symptoms (vertigo, balance problems, ear ringing, double vision).
Conclusion: Assessing a broader range of headache-associated symptoms reveals clustering of symptomatology and a strong relationship with headache burden.
Keywords: Pediatric; diagnosis; headache; headache-associated symptoms; migraine.
Figures


References
-
- Harriott AM and Schwedt TJ. Migraine is associated with altered processing of sensory stimuli. Curr Pain Headache Rep 2014; 18: 1–7. - PubMed
-
- Hershey AD, Winner P, Kabbouche MA, et al. Use of the ICHD-ii criteria in the diagnosis of pediatric migraine. Headache J Head Face Pain 2005; 45: 1288–1297. - PubMed
-
- International Headache Society. The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018; 38: 1–211. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
