

Early Pregnancy Systolic Blood Pressure Patterns Predict Early- and Later-Onset Preeclampsia and Gestational Hypertension Among Ostensibly Low-to-Moderate Risk Groups
- PMID: 37435795
- PMCID: PMC10492985
- DOI: 10.1161/JAHA.123.029617
Early Pregnancy Systolic Blood Pressure Patterns Predict Early- and Later-Onset Preeclampsia and Gestational Hypertension Among Ostensibly Low-to-Moderate Risk Groups
Abstract
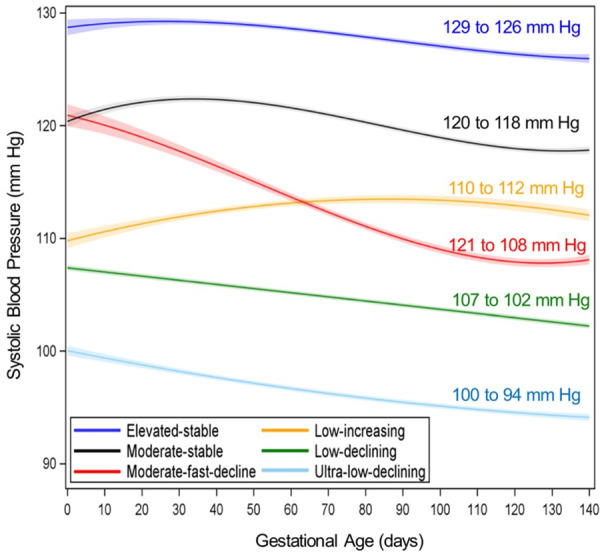
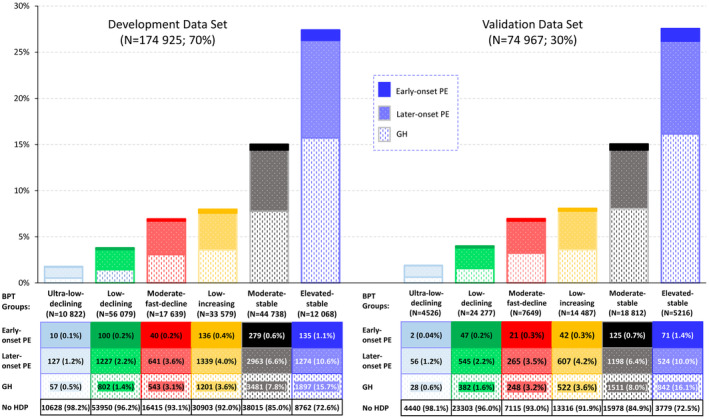
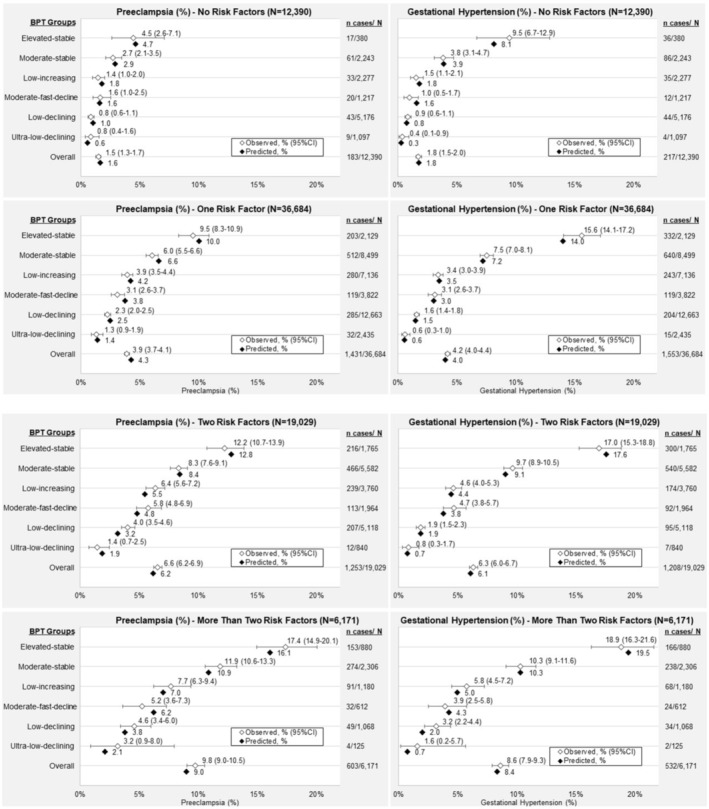
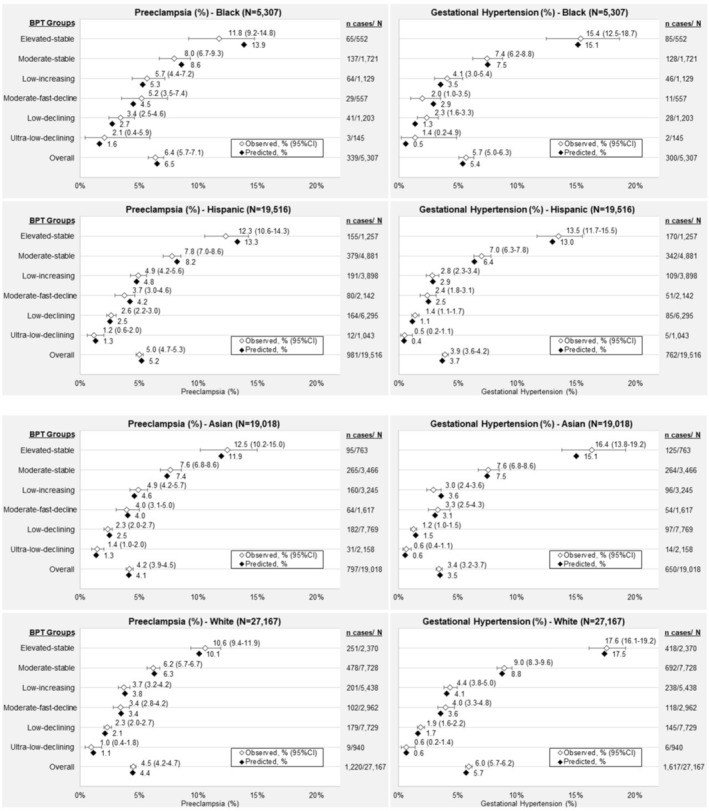
Background Clinical risk factors, a single blood pressure (BP) measurement, current biomarkers, and biophysical parameters can effectively identify risk of early-onset preeclampsia but have limited ability to predict later-onset preeclampsia and gestational hypertension. Clinical BP patterns hold promise to improve early risk stratification for hypertensive disorders of pregnancy. Methods and Results After excluding preexisting hypertension, heart, kidney, or liver disease, or prior preeclampsia, the retrospective cohort (n=249 892) all had systolic BP <140 mm Hg and diastolic BP <90 mm Hg or a single BP elevation ≤20 weeks' gestation, prenatal care at <14 weeks' gestation, and a still or live birth delivery at Kaiser Permanente Northern California hospitals (2009-2019). The sample was randomly split into development (N=174 925; 70%) and validation (n=74 967; 30%) data sets. Predictive performance of multinomial logistic regression models for early-onset (<34 weeks) preeclampsia, later-onset (≥34 weeks) preeclampsia, and gestational hypertension was evaluated in the validation data set. There were 1008 (0.4%), 10 766 (4.3%), and 11 514 (4.6%) patients with early-onset preeclampsia, later-onset preeclampsia, and gestation hypertension, respectively. Models with 6 systolic BP trajectory groups (0-20 weeks' gestation) plus standard clinical risk factors performed substantially better than risk factors alone to predict early- and later-onset preeclampsia and gestational hypertension, with C-statistics (95% CIs) of 0.747 (0.720-0.775), 0.730 (0.722-0.739), and 0.768 (0.761-0.776) versus 0.688 (0.659-0.717), 0.695 (0.686-0.704) and 0.692 (0.683-0.701), respectively, with excellent calibration (Hosmer-Lemeshow P=0.99, 0.99, and 0.74, respectively). Conclusions Early pregnancy BP patterns up to 20 weeks' gestation plus clinical, social, and behavioral factors more accurately discriminate hypertensive disorders of pregnancy risk among low-to-moderate risk pregnancies. Early pregnancy BP trajectories improve risk stratification to reveal higher-risk individuals hidden within ostensibly low-to-moderate risk groups and lower-risk individuals considered at higher risk by US Preventive Services Task Force criteria.
Keywords: blood pressure; hypertensive disorders; longitudinal trajectory analysis; prediction; preeclampsia; pregnancy; risk stratification.
Figures
Comment in
-
Are Early Pregnancy Blood Pressure Patterns a Crystal Ball for Predicting Preeclampsia and Gestational Hypertension?J Am Heart Assoc. 2023 Aug;12(15):e031068. doi: 10.1161/JAHA.123.031068. Epub 2023 Jul 12. J Am Heart Assoc. 2023. PMID: 37435794 Free PMC article. No abstract available.
References
-
- Garovic VD, Dechend R, Easterling T, Karumanchi SA, McMurtry Baird S, Magee LA, Rana S, Vermunt JV, August P. Hypertension in pregnancy: diagnosis, blood pressure goals, and pharmacotherapy: a scientific statement from the American Heart Association. Hypertension. 2022;79:e21–e41. doi: 10.1161/HYP.0000000000000208 - DOI - PMC - PubMed
-
- US Preventive Services Task Force; Bibbins‐Domingo K, Grossman DC, Curry SJ, Barry MJ, Davidson KW, Doubeni CA, Epling JW Jr, Kemper AR, Krist AH, Kurth AE, et al. Screening for preeclampsia: US Preventive Services Task Force recommendation statement. JAMA. 2017;317:1661–1667. doi: 10.1001/jama.2017.3439 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
