

Infigratinib, a selective FGFR1-3 tyrosine kinase inhibitor, alters dentoalveolar development at high doses
- PMID: 37435833
- PMCID: PMC10784415
- DOI: 10.1002/dvdy.642
Infigratinib, a selective FGFR1-3 tyrosine kinase inhibitor, alters dentoalveolar development at high doses
Abstract
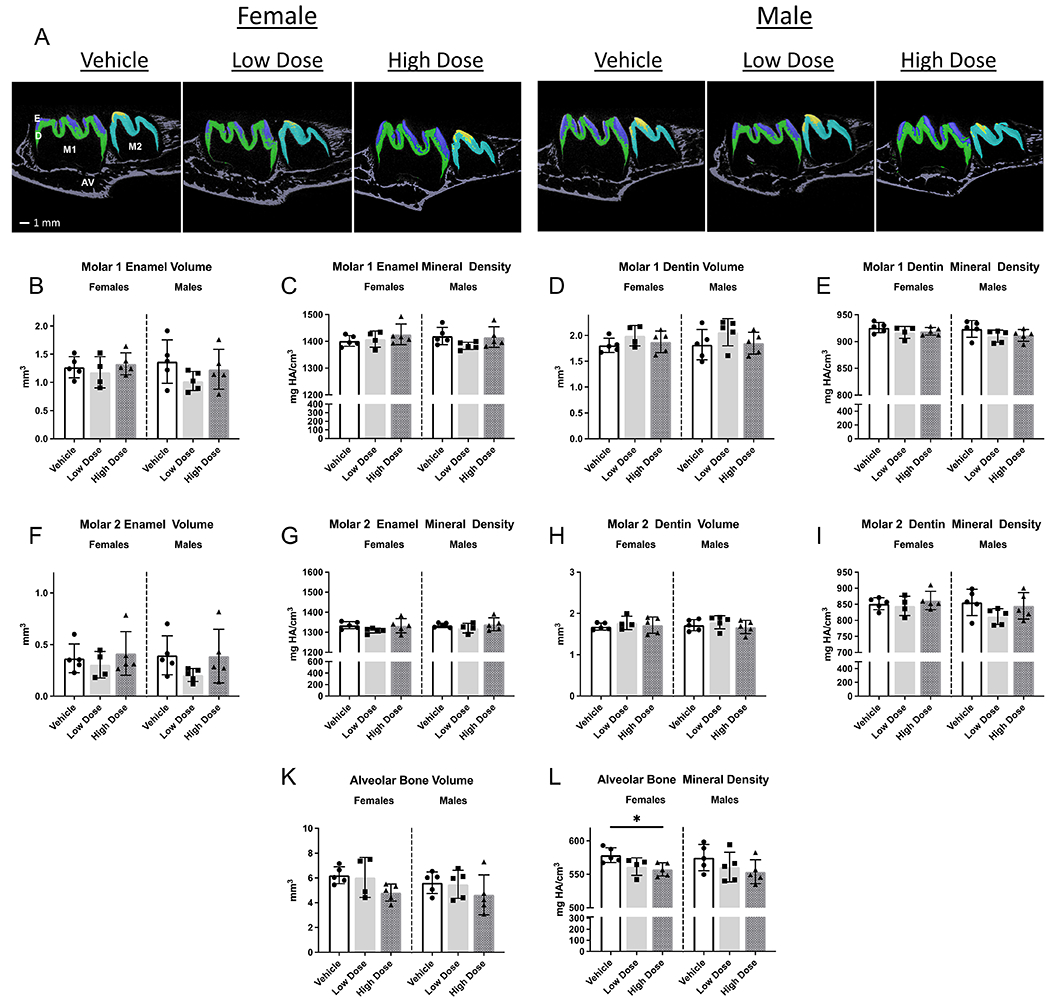
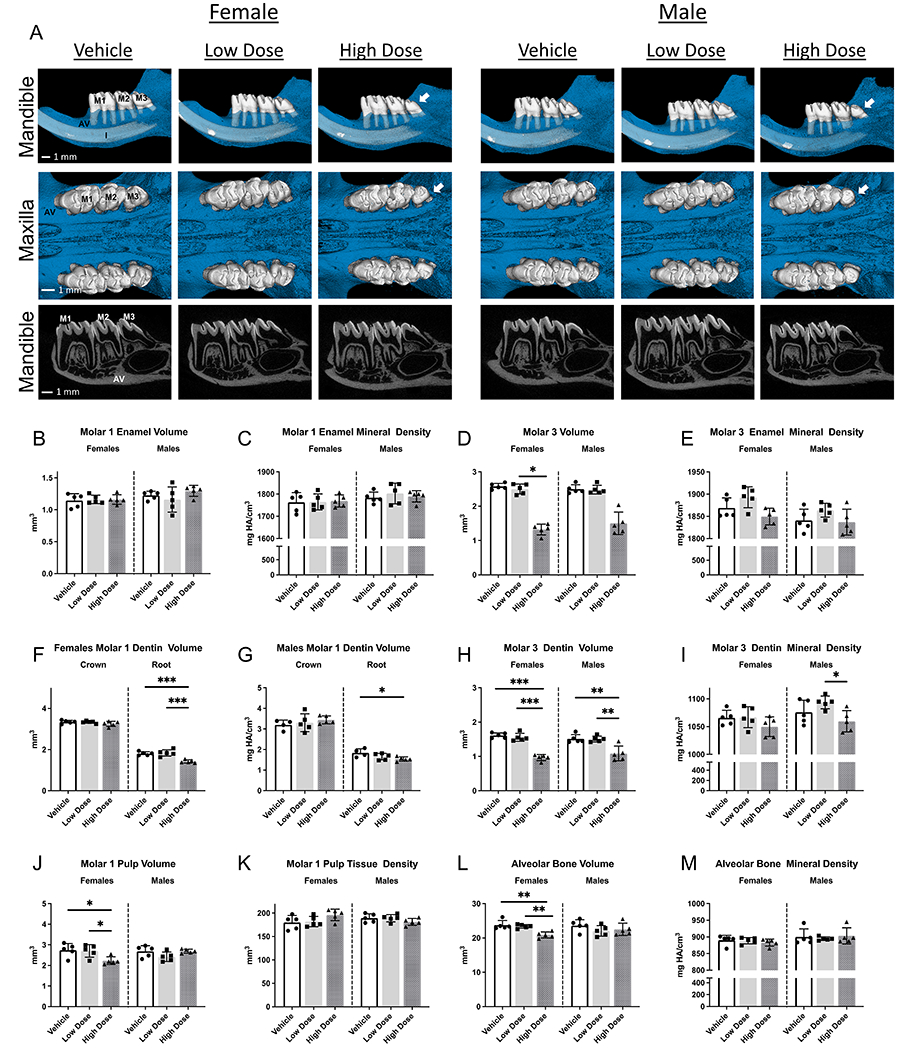
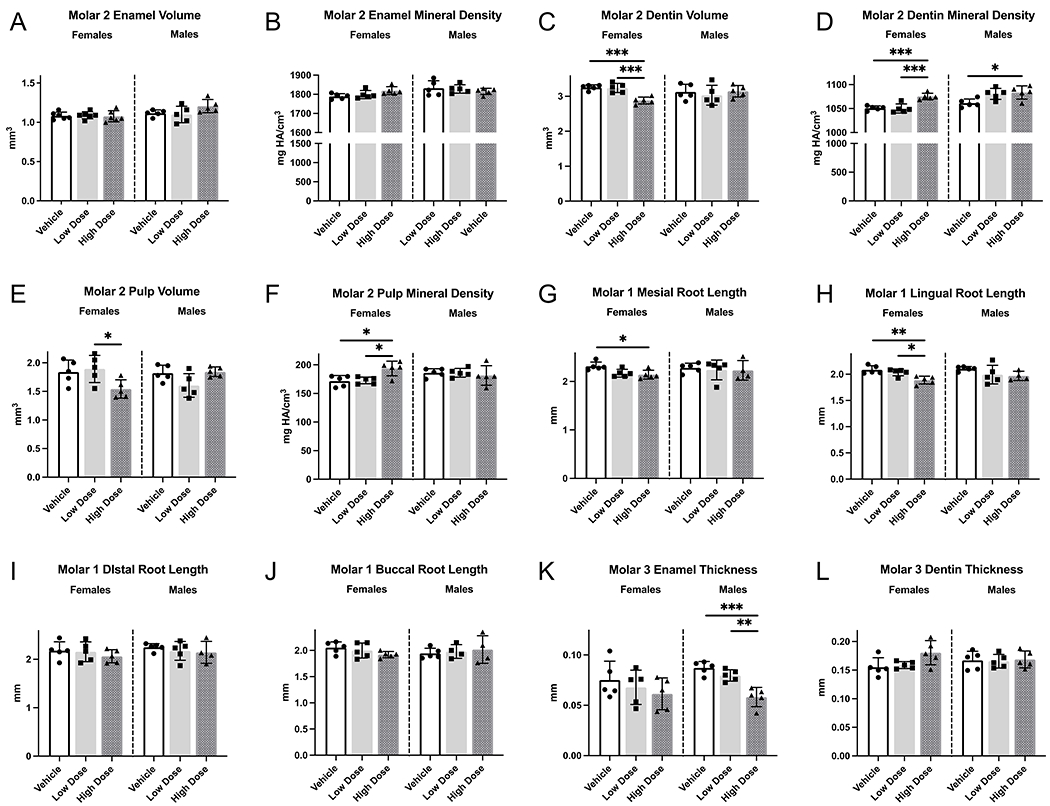
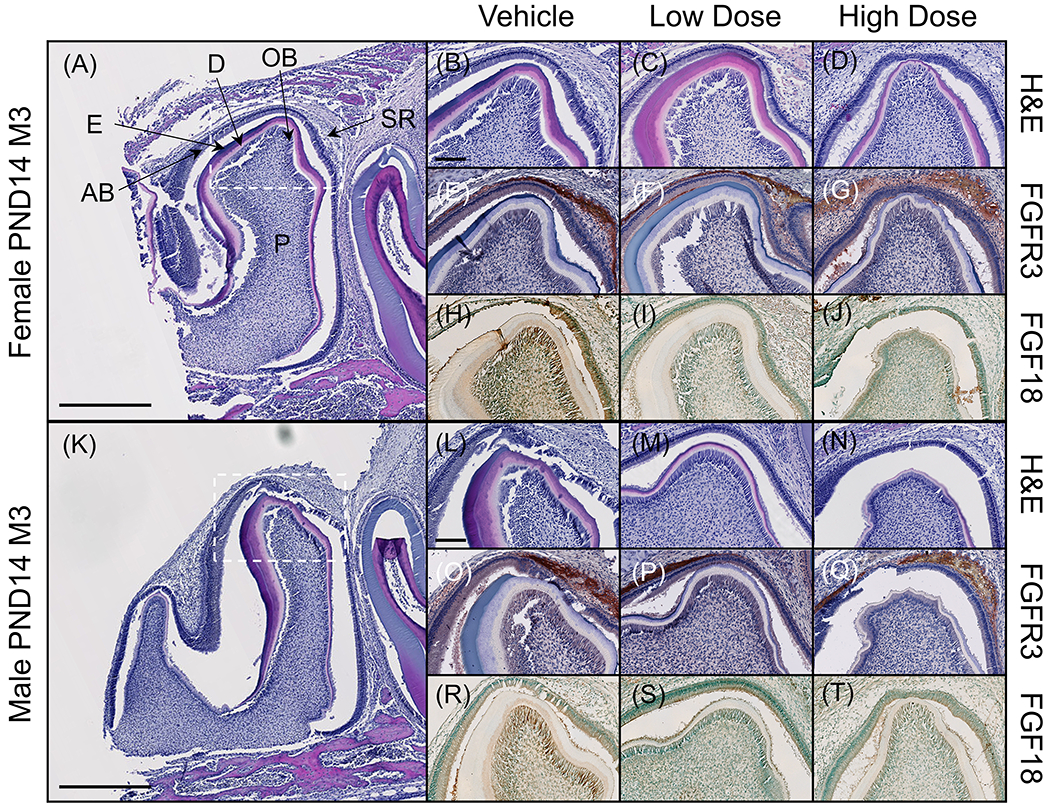
Background: Fibroblast growth factor receptor-3 (FGFR3) gain-of-function mutations are linked to achondroplasia. Infigratinib, a FGFR1-3 tyrosine kinase inhibitor, improves skeletal growth in an achondroplasia mouse model. FGFs and their receptors have critical roles in developing teeth, yet effects of infigratinib on tooth development have not been assessed. Dentoalveolar and craniofacial phenotype of Wistar rats dosed with low (0.1 mg/kg) and high (1.0 mg/kg) dose infigratinib were evaluated using micro-computed tomography, histology, and immunohistochemistry.
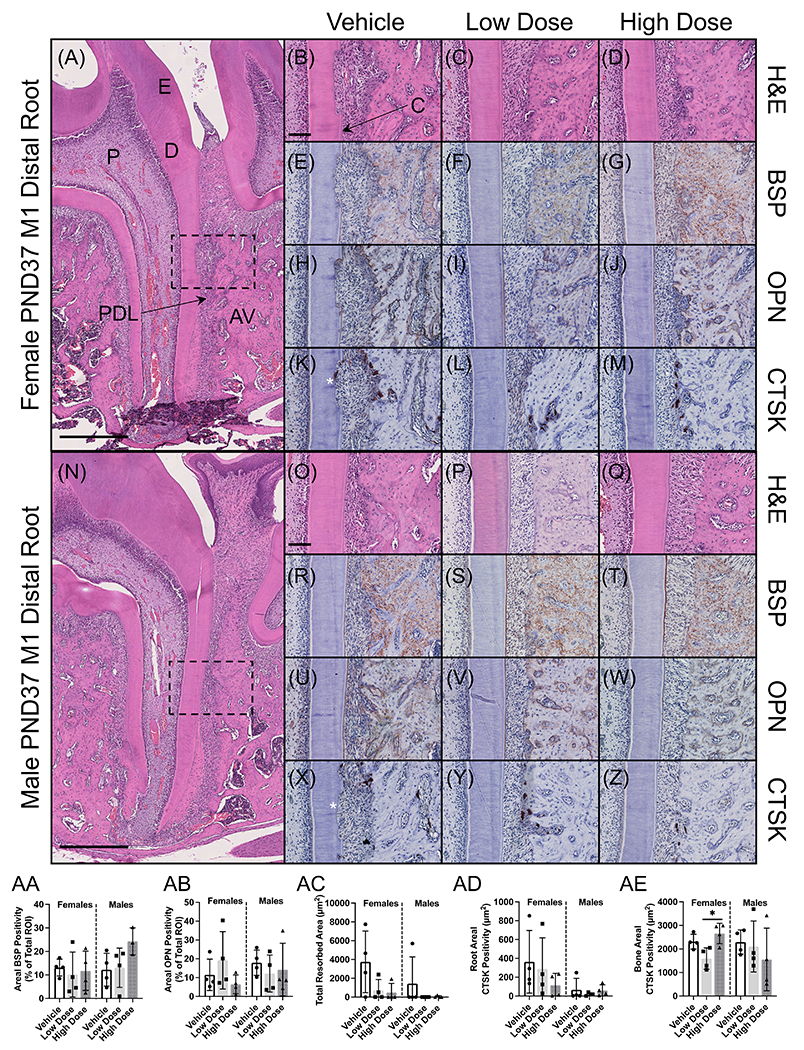
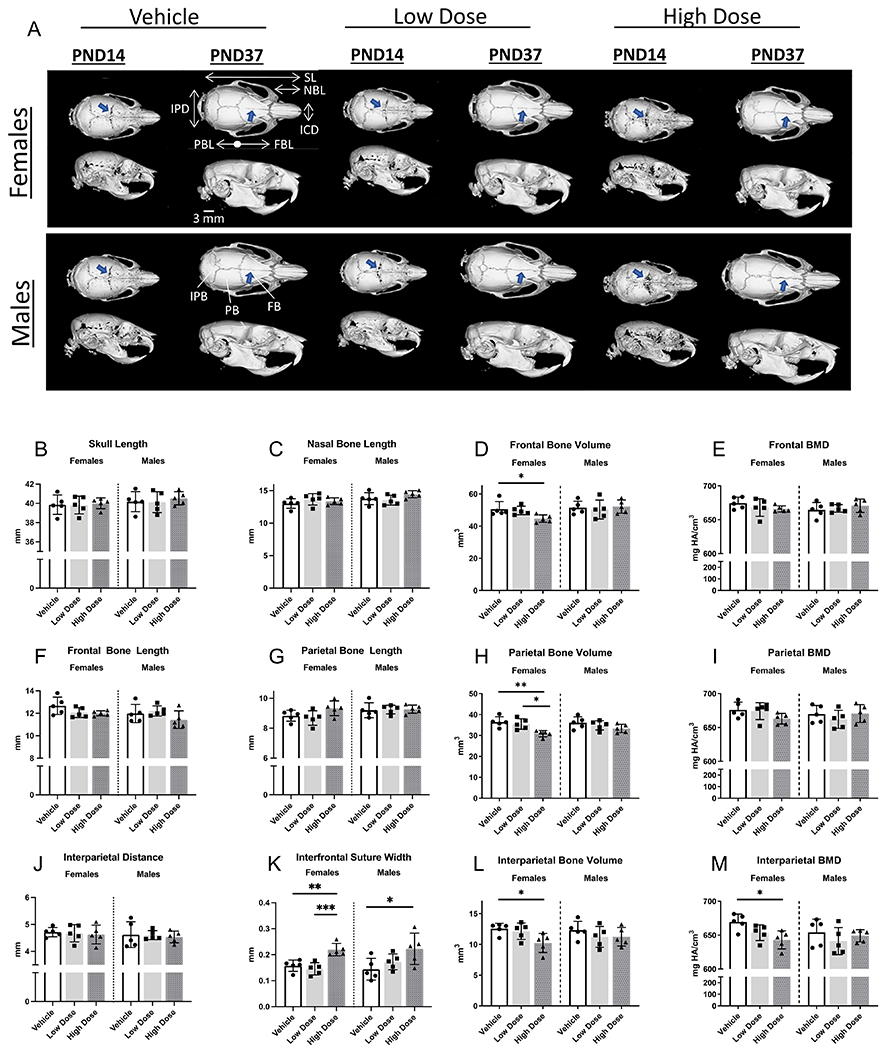
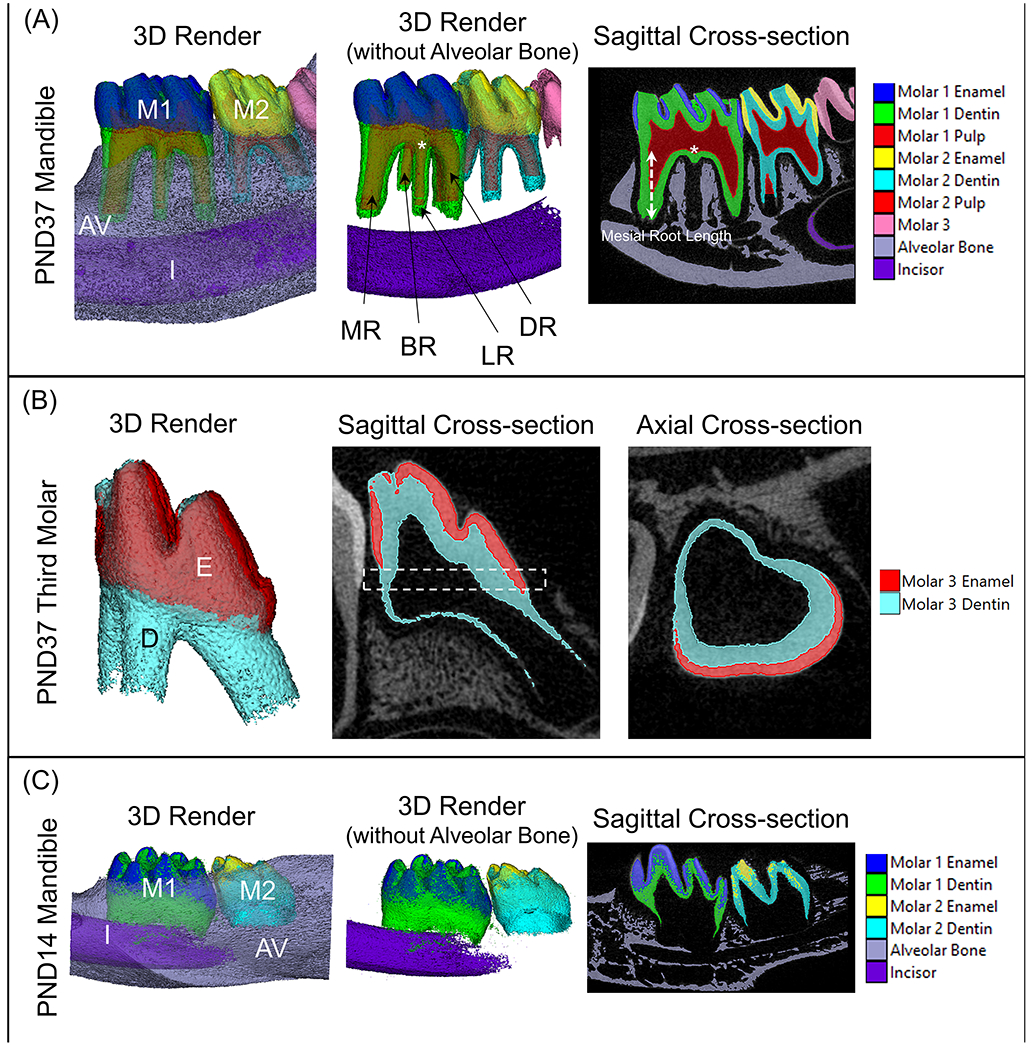
Results: Mandibular third molars were reduced in size and exhibited aberrant crown and root morphology in 100% of female rats and 80% of male rats at high doses. FGFR3 and FGF18 immunolocalization and extracellular matrix protein expression were unaffected, but cathepsin K (CTSK) was altered by infigratinib. Cranial vault bones exhibited alterations in dimension, volume, and density that were more pronounced in females. In both sexes, interfrontal sutures were significantly more patent with high dose vs vehicle.
Conclusions: High dose infigratinib administered to rats during early stages affects dental and craniofacial development. Changes in CTSK from infigratinib in female rats suggest FGFR roles in bone homeostasis. While dental and craniofacial disruptions are not expected at therapeutic doses, our findings confirm the importance of dental monitoring in clinical studies.
Keywords: bone; fibroblast growth factor receptor; mineralized tissue/development; tooth development.
© 2023 American Association for Anatomy.
Figures
References
-
- Legare JM. Achondroplasia. In: Adam MP, Ardinger HH, Pagon RA, et al. , eds. GeneReviews®. University of Washington, Seattle; 1993. Accessed March 1, 2022. http://www.ncbi.nlm.nih.gov/books/NBK1152/ - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
