

A Real-Time Neurophysiologic Stress Test for the Aging Brain: Novel Perioperative and ICU Applications of EEG in Older Surgical Patients
- PMID: 37436580
- PMCID: PMC10457272
- DOI: 10.1007/s13311-023-01401-4
A Real-Time Neurophysiologic Stress Test for the Aging Brain: Novel Perioperative and ICU Applications of EEG in Older Surgical Patients
Erratum in
-
Corrigendum to "A real-time neurophysiologic stress test for the aging brain: Novel perioperative and ICU applications of EEG in older surgical patients" Neurotherapeutics 20 (4) (2023) 975-1000.Neurotherapeutics. 2024 Oct;21(6):e00473. doi: 10.1016/j.neurot.2024.e00473. Epub 2024 Oct 31. Neurotherapeutics. 2024. PMID: 39482181 Free PMC article. No abstract available.
Abstract
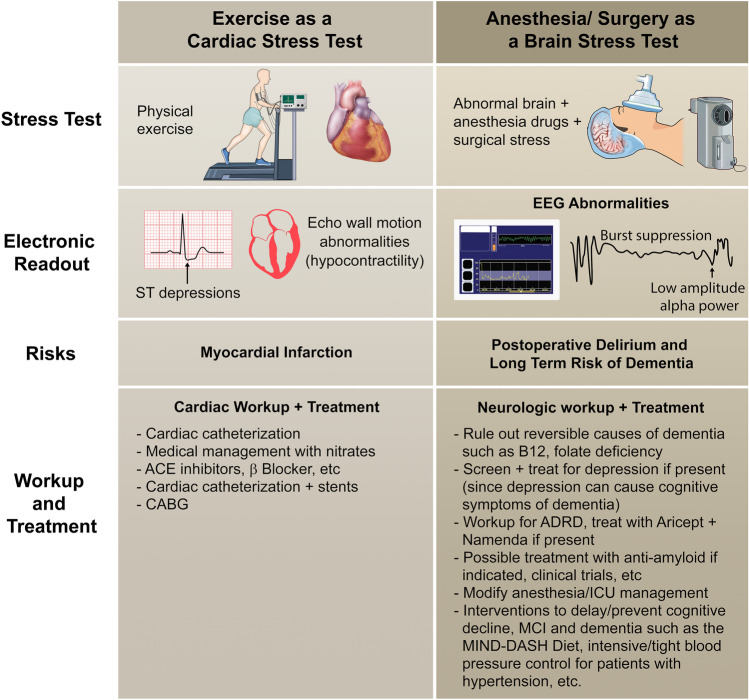
As of 2022, individuals age 65 and older represent approximately 10% of the global population [1], and older adults make up more than one third of anesthesia and surgical cases in developed countries [2, 3]. With approximately > 234 million major surgical procedures performed annually worldwide [4], this suggests that > 70 million surgeries are performed on older adults across the globe each year. The most common postoperative complications seen in these older surgical patients are perioperative neurocognitive disorders including postoperative delirium, which are associated with an increased risk for mortality [5], greater economic burden [6, 7], and greater risk for developing long-term cognitive decline [8] such as Alzheimer's disease and/or related dementias (ADRD). Thus, anesthesia, surgery, and postoperative hospitalization have been viewed as a biological "stress test" for the aging brain, in which postoperative delirium indicates a failed stress test and consequent risk for later cognitive decline (see Fig. 3). Further, it has been hypothesized that interventions that prevent postoperative delirium might reduce the risk of long-term cognitive decline. Recent advances suggest that rather than waiting for the development of postoperative delirium to indicate whether a patient "passed" or "failed" this stress test, the status of the brain can be monitored in real-time via electroencephalography (EEG) in the perioperative period. Beyond the traditional intraoperative use of EEG monitoring for anesthetic titration, perioperative EEG may be a viable tool for identifying waveforms indicative of reduced brain integrity and potential risk for postoperative delirium and long-term cognitive decline. In principle, research incorporating routine perioperative EEG monitoring may provide insight into neuronal patterns of dysfunction associated with risk of postoperative delirium, long-term cognitive decline, or even specific types of aging-related neurodegenerative disease pathology. This research would accelerate our understanding of which waveforms or neuronal patterns necessitate diagnostic workup and intervention in the perioperative period, which could potentially reduce postoperative delirium and/or dementia risk. Thus, here we present recommendations for the use of perioperative EEG as a "predictor" of delirium and perioperative cognitive decline in older surgical patients.
Keywords: Alzheimer’s disease; Anesthesia; Cognitive impairment; Delirium; Dementia; Neurophysiology.
© 2023. The Author(s).
Conflict of interest statement
Dr. Berger acknowledges funding from Minnetronix, Inc. (St. Paul, Minnesota), for a project unrelated to the subject matter of this review. Dr Berger has received material support (i.e., electroencephalogram monitor loans) for a postoperative recovery study in older adults from Masimo, Inc. (Irvine, California), and has attended Masimo peer-to-peer EEG education events (for which his honorarium was donated at his request to the Foundation for Anesthesia Education and Research). Dr. Berger has also received legal consulting fees related to postoperative cognition in an older adult. The other authors declare no competing interests.
Figures

References
-
- UN. World Population Prospects 2022: Ten key messages. In: Department of Economic and Social Affairs PD, editor. 2022.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
