

Adiposity and risk of oesophageal cancer subtypes in the Million Women Study
- PMID: 37437897
- PMCID: PMC10749780
- DOI: 10.1093/ije/dyad094
Adiposity and risk of oesophageal cancer subtypes in the Million Women Study
Abstract
Background: The strong association of body mass index (BMI) with increased oesophageal adenocarcinoma risk is established, but its relationship with oesophageal squamous cell carcinoma is less clear. There is little evidence regarding the association of abdominal adiposity with either subtype.
Methods: In a large prospective cohort of women in the UK, mean age 56.2 [standard deviation (SD) = 4.9] years, we investigated the risk of oesophageal adenocarcinoma and squamous cell carcinoma in relation to self-reported BMI, waist circumference (WC) and waist-hip ratio (WHR), using Cox regression to estimate adjusted relative risks (RR) and 95% confidence intervals (CIs), taking account of potential reverse causation bias.
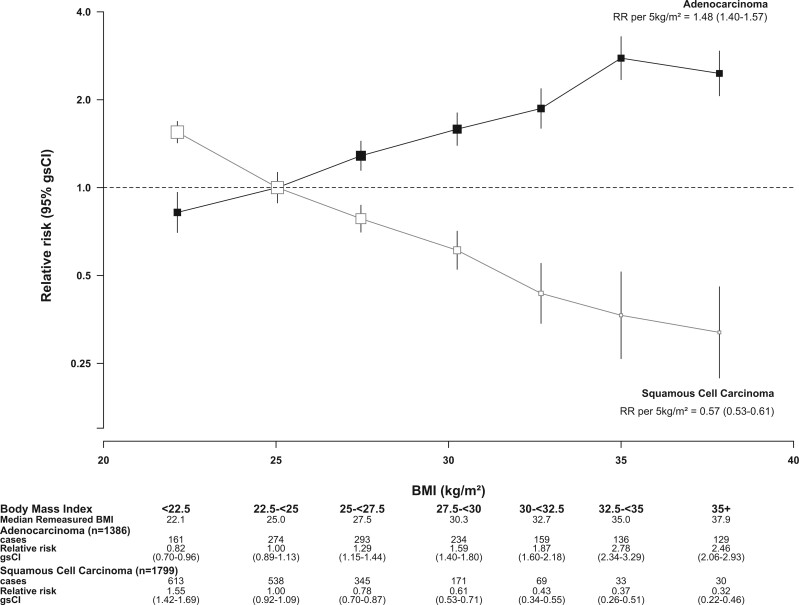
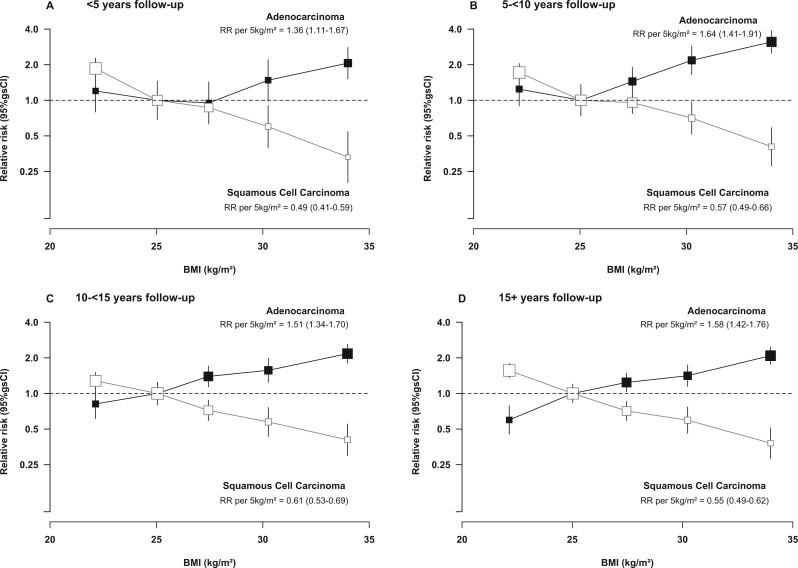
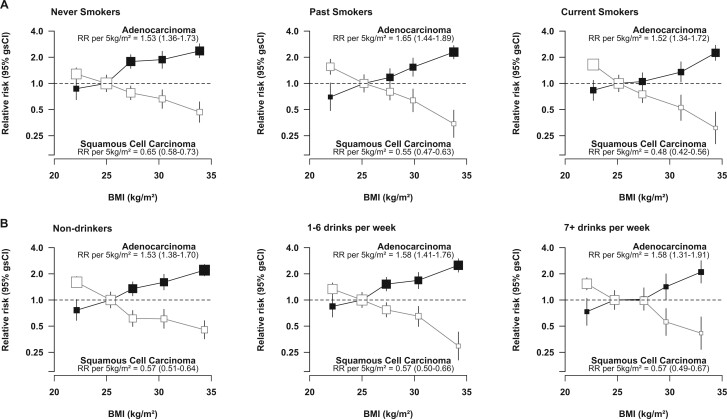
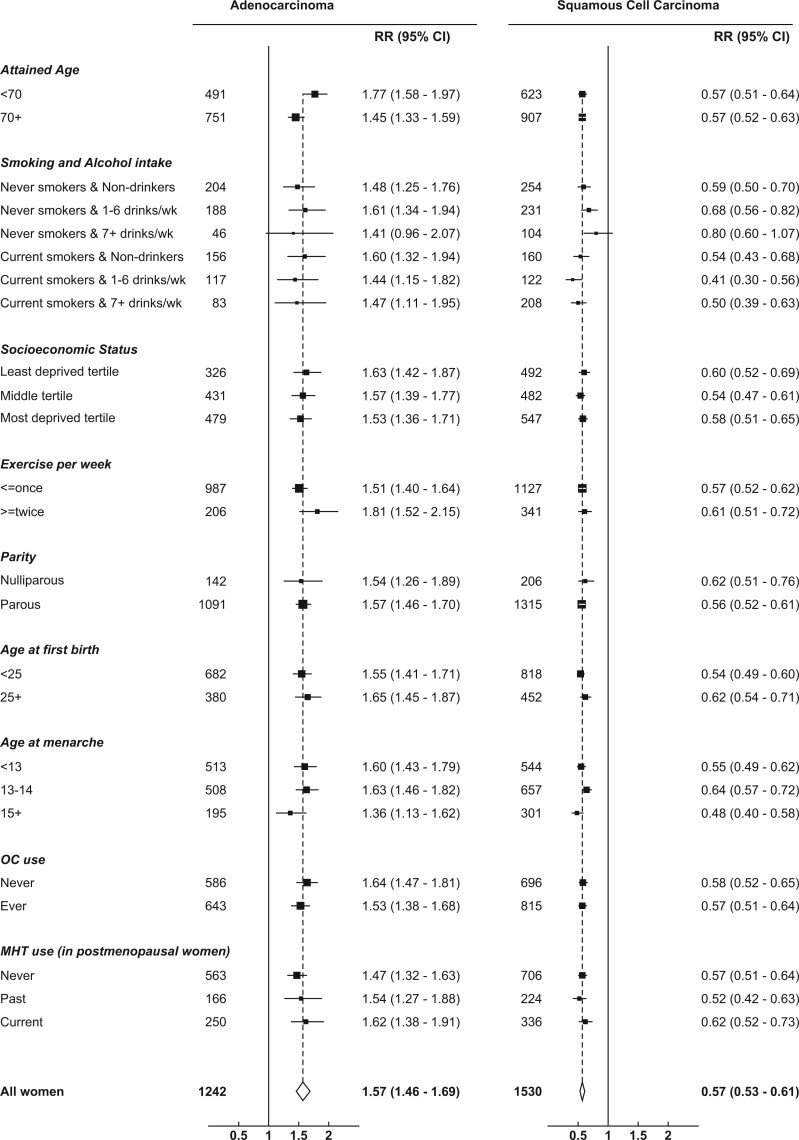
Results: During mean follow-up of 17.7 (SD = 4.9) years, 1386 adenocarcinomas and 1799 squamous cell carcinomas of the oesophagus were registered among 1 255 529 women. Compared with women of BMI 22.5 to <25 kg/m2, those with BMI ≥35 kg/m2 had a 2.5-fold risk of adenocarcinoma (adjusted RR = 2.46, 95% CI = 1.99-3.05) and an almost 70% reduction in risk of squamous cell carcinoma (RR = 0.32, 95% CI = 0.22-0.46). These associations were broadly similar in each 5-year follow-up period, and were evident in both never and ever smokers, although somewhat stronger for squamous cell carcinoma among current and past smokers than in never smokers (Pheterogeneity = 0.007). After controlling for BMI, WC and WHR were associated with risk of squamous cell carcinoma but not adenocarcinoma.
Conclusions: In this population of middle-aged women, there was robust evidence that greater BMI is associated with an increased risk of oesophageal adenocarcinoma and a reduced risk of squamous cell carcinoma.
Keywords: Oesophageal cancer; abdominal adiposity; adenocarcinoma; body mass index; squamous cell carcinoma.
© The Author(s) 2023. Published by Oxford University Press on behalf of the International Epidemiological Association.
Conflict of interest statement
None declared.
Figures
References
-
- Sung H, Ferlay J, Siegel RL. et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71:209–49. - PubMed
-
- Arnold M, Ferlay J, van Berge Henegouwen MI. et al. Global burden of oesophageal and gastric cancer by histology and subsite in 2018. Gut 2020;69:1564–71. - PubMed
-
- NHS. NHS Cancer Data - Get Data Out 2022. https://www.cancerdata.nhs.uk/getdataout/oes (17 May 2022, date last accessed).
-
- Engeland A, Tretli S, Bjorge T.. Height and body mass index in relation to esophageal cancer; 23-year follow-up of two million Norwegian men and women. Cancer Causes Control 2004;15:837–43. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
