

Staged or simultaneous operations for ventriculoperitoneal shunt and cranioplasty: Evidence from a meta-analysis
- PMID: 37438995
- PMCID: PMC10580328
- DOI: 10.1111/cns.14347
Staged or simultaneous operations for ventriculoperitoneal shunt and cranioplasty: Evidence from a meta-analysis
Abstract
Objective: To date, there is no consensus on the surgery strategies of cranioplasty (CP) and ventriculoperitoneal shunt (VPS) placement. This meta-analysis aimed to investigate the safety of staged and simultaneous operation in patients with comorbid cranial defects with hydrocephalus to inform future surgery protocols.
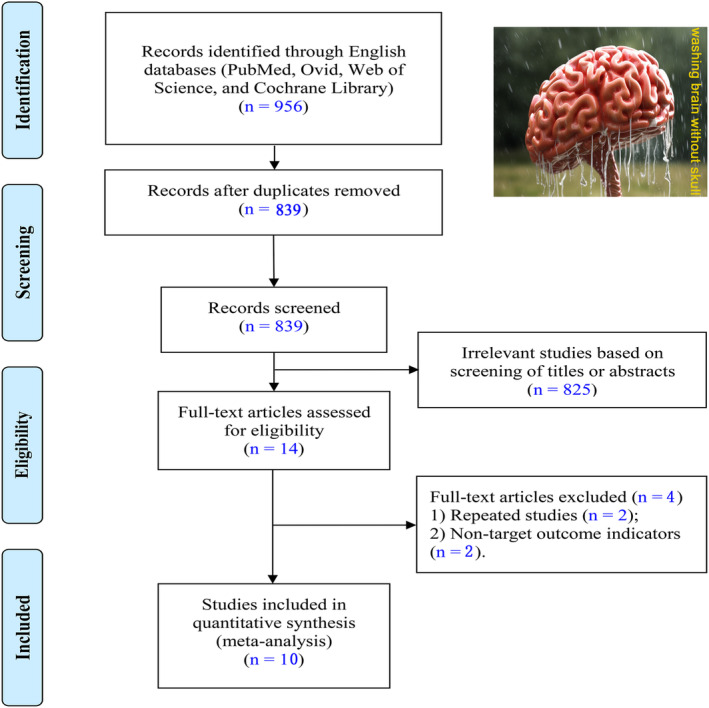
Methods: A meta-analysis of PubMed, Ovid, Web of Science, and Cochrane Library databases from the inception dates to February 8, 2023 adherent to PRISMA guidelines was conducted. The pooled analyses were conducted using RevMan 5.3 software. The outcomes included postoperative infection, reoperation, shunt obstruction, hematoma, and subdural effusion.
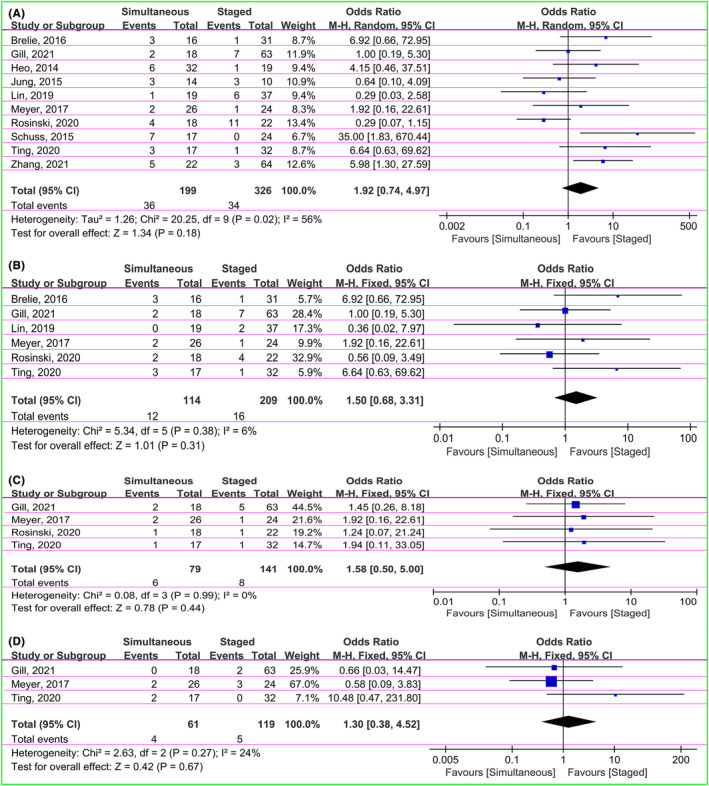
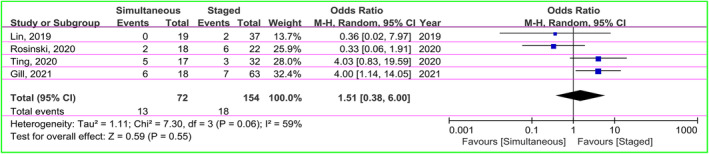
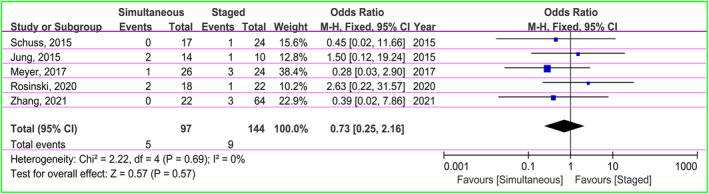
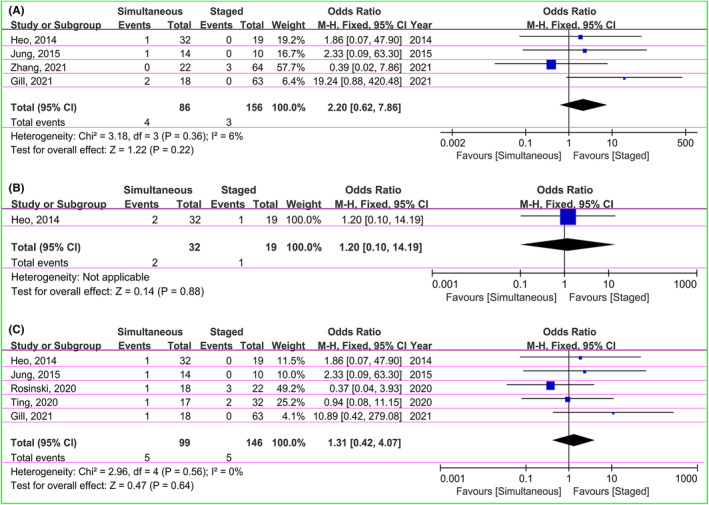
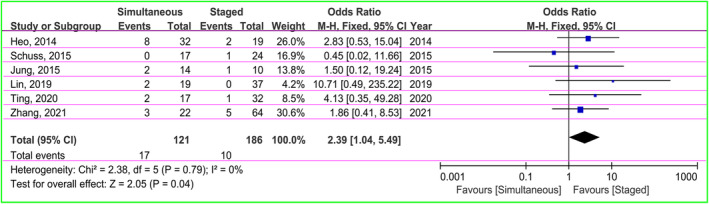
Results: Of the 956 studies initially retrieved, 10 articles encompassing 515 patients were included. Among the total patients, 193 (37.48%) and 322 (62.52%), respectively, underwent simultaneous and staged surgeries. The finding of pooled analysis indicated that staged surgery was associated with lower rate of subdural effusion (14% in the simultaneous groups vs. 5.4% in the staged groups; OR = 2.39, 95% CI: 1.04-5.49, p = 0.04). However, there were no significant differences in overall infection (OR = 1.92, 95% CI: 0.74-4.97, p = 0.18), central nervous system infection (OR = 1.50, 95% CI: 0.68-3.31, p = 0.31), cranioplasty infection (OR = 1.58, 95% CI: 0.50-5.00, p = 0.44), shunt infection (OR = 1.30, 95% CI: 0.38-4.52, p = 0.67), reoperation (OR = 1.51, 95% CI: 0.38-6.00, p = 0.55), shunt obstruction (OR = 0.73, 95% CI: 0.25-2.16, p = 0.57), epidural hematoma (OR = 2.20, 95% CI: 0.62-7.86, p = 0.22), subdural hematoma (OR = 1.20, 95% CI: 0.10-14.19, p = 0.88), and intracranial hematoma (OR = 1.31, 95% CI: 0.42-4.07, p = 0.64). Moreover, subgroup analysis failed to yield new insights.
Conclusions: Staged surgery is associated with a lower rate of postoperative subdural effusion. However, from the evidence of sensitivity analysis, this result is not stable. Therefore, our conclusion should be viewed with caution, and neurosurgeons in practice should make individualized decisions based on each patient's condition and cerebrospinal fluid tap test.
Keywords: complications; craniectomy; cranioplasty; hydrocephalus; ventriculoperitoneal shunt.
© 2023 The Authors. CNS Neuroscience & Therapeutics Published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Simultaneous cranioplasty and ventriculoperitoneal shunt placement in patients with traumatic brain injury undergoing unilateral decompressive craniectomy.J Clin Neurosci. 2020 Sep;79:45-50. doi: 10.1016/j.jocn.2020.07.015. Epub 2020 Aug 5. J Clin Neurosci. 2020. PMID: 33070916
-
Cranioplasty and Ventriculoperitoneal Shunt Placement after Decompressive Craniectomy: Staged Surgery Is Associated with Fewer Postoperative Complications.World Neurosurg. 2015 Oct;84(4):1051-4. doi: 10.1016/j.wneu.2015.05.066. Epub 2015 Jun 11. World Neurosurg. 2015. PMID: 26072458
-
Evaluation of simultaneous cranioplasty and ventriculoperitoneal shunt procedures.J Neurosurg. 2014 Aug;121(2):313-8. doi: 10.3171/2014.2.JNS131480. Epub 2014 Mar 21. J Neurosurg. 2014. PMID: 24655097
-
To shunt or not to shunt when closing myelomeningocele? A systematic review and meta-analysis of simultaneous versus delayed ventriculoperitoneal shunt placement in neonates undergoing myelomeningocele closure.J Neurosurg Pediatr. 2024 Aug 9;34(5):452-461. doi: 10.3171/2024.5.PEDS23600. Print 2024 Nov 1. J Neurosurg Pediatr. 2024. PMID: 39126714
-
Endoscopic Third Ventriculostomy versus Ventriculoperitoneal Shunt in Patients with Obstructive Hydrocephalus: Meta-Analysis of Randomized Controlled Trials.World Neurosurg. 2019 Sep;129:334-340. doi: 10.1016/j.wneu.2019.04.255. Epub 2019 May 25. World Neurosurg. 2019. PMID: 31136836 Review.
Cited by
-
Timing of cerebrospinal fluid diversion with ventriculoperitoneal shunt placement in cranioplasty reconstruction: A systematic review and meta-analysis.Surg Neurol Int. 2025 Mar 28;16:114. doi: 10.25259/SNI_771_2024. eCollection 2025. Surg Neurol Int. 2025. PMID: 40206743 Free PMC article.
-
The role and mechanism of immunotherapy in pediatric subdural Effusion:Case reports and literature review.Heliyon. 2024 Jun 28;10(13):e33732. doi: 10.1016/j.heliyon.2024.e33732. eCollection 2024 Jul 15. Heliyon. 2024. PMID: 39071687 Free PMC article.
References
-
- Kocher T. Hirnerschütterung, Hirndruck und chirurgische Eingriffe bei Hirnkrankheiten. Alfred Hölder; 1901.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
