

A Medial Approach That Provides Ample Exposure of the Coronoid for Fracture Management
- PMID: 37439145
- PMCID: PMC10651265
- DOI: 10.1097/BTH.0000000000000444
A Medial Approach That Provides Ample Exposure of the Coronoid for Fracture Management
Abstract
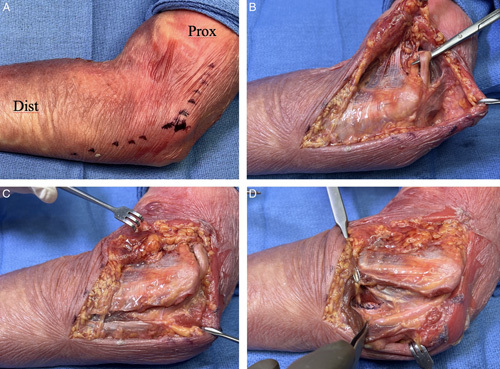
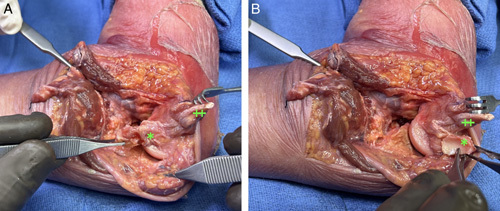
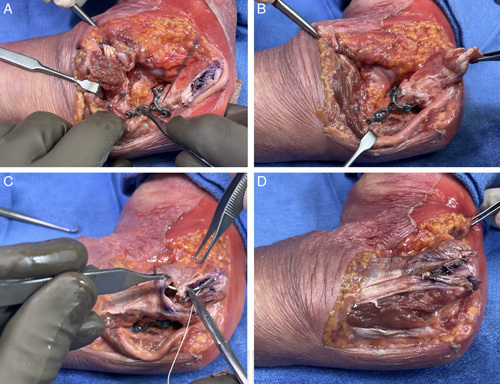
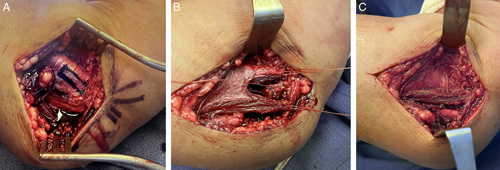
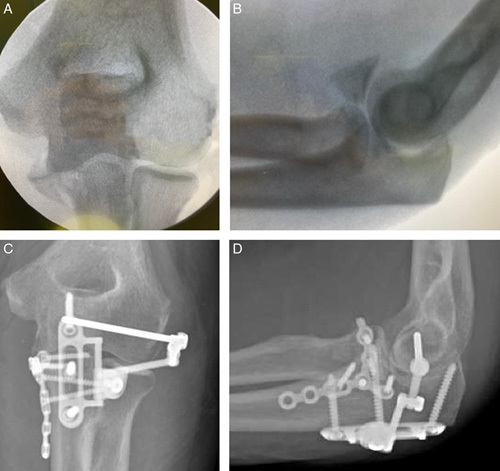
We describe a medial approach to the coronoid where the flexor-pronator mass is released from its humeral origin by creating a proximally based tendinous flap. This technique facilitates access to the coronoid, preservation of the medial collateral ligament origin, and repair of the flexor-pronator mass. This approach has utility for all coronoid fracture variations but especially the O'Driscoll anteromedial subtype 3, which includes fractures of the sublime tubercle, the anteromedial facet, and the coronoid tip.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
Conflicts of Interest and Source of Funding: J.L.O. discloses patents 8506606 and 8608741 issued to Skeletal Dynamics. Irrevocable trusts of which J.L.O. and his family members are the beneficiaries and own stock in Skeletal Dynamics, and Skeletal Dynamics reimburses expenses when J.L.O. speaks or presents on the company’s behalf. F.R., R.R.L.G., N.A.H., and D.M.M. disclose a relationship with Skeletal Dynamics that includes consulting and speaker’s bureau. D.M.M. discloses a relationship with Axogen that includes the speaker’s bureau. For the remaining author none were declared.
Figures

References
-
- O’Driscoll SW. Classification and evaluation of recurrent instability of the elbow. Clin Orthop Relat Res. 2000;370:34–43. - PubMed
-
- O’Driscoll SW, Jupiter JB, Cohen MS, et al. . Difficult elbow fractures: pearls and pitfalls. Instr Course Lect. 2003;52:113–134. - PubMed
-
- Hotchkiss RN, Kasparyan NG. The medial “over the top” approach to the elbow. Tech Orthop. 2000;15:105–112.
-
- Taylor TK, Scham SM. A posteromedial approach to the proximal end of the ulna for the internal fixation of olecranon fractures. J Trauma. 1969;9:594–602. - PubMed
-
- Bates T, Lynch TB, Achay J, et al. . Medial elbow exposure: Modified Taylor-Scham Versus Flexor Carpi Ulnaris-Split. J Orthop Trauma. 2023;37:e63–e67. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
