

Low-Dose 0.01% Atropine Eye Drops vs Placebo for Myopia Control: A Randomized Clinical Trial
- PMID: 37440213
- PMCID: PMC10346510
- DOI: 10.1001/jamaophthalmol.2023.2855
Low-Dose 0.01% Atropine Eye Drops vs Placebo for Myopia Control: A Randomized Clinical Trial
Abstract
Importance: Controlling myopia progression is of interest worldwide. Low-dose atropine eye drops have slowed progression in children in East Asia.
Objective: To compare atropine, 0.01%, eye drops with placebo for slowing myopia progression in US children.
Design, setting, and participants: This was a randomized placebo-controlled, double-masked, clinical trial conducted from June 2018 to September 2022. Children aged 5 to 12 years were recruited from 12 community- and institution-based practices in the US. Participating children had low to moderate bilateral myopia (-1.00 diopters [D] to -6.00 D spherical equivalent refractive error [SER]).
Intervention: Eligible children were randomly assigned 2:1 to 1 eye drop of atropine, 0.01%, nightly or 1 drop of placebo. Treatment was for 24 months followed by 6 months of observation.
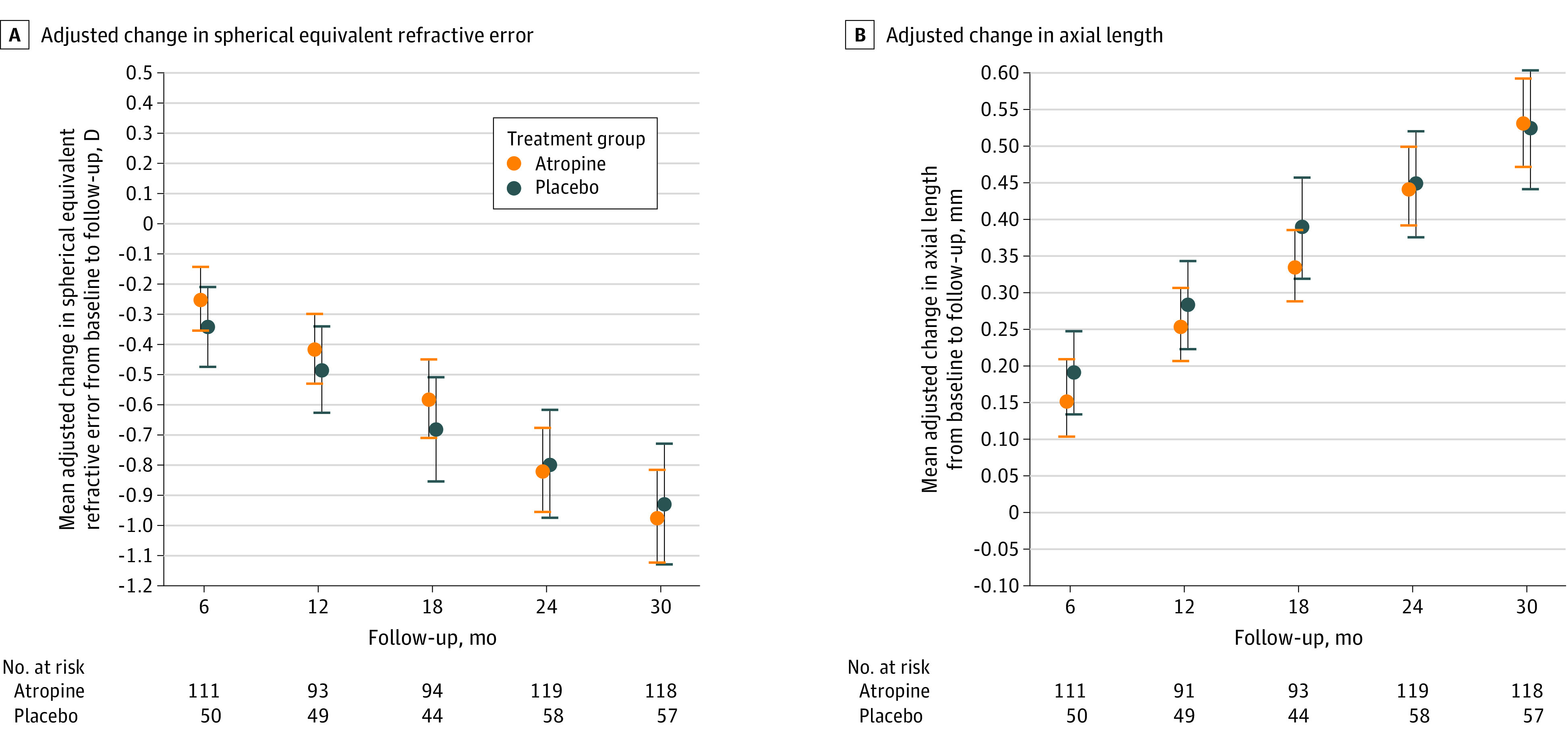
Main outcome and measures: Automated cycloplegic refraction was performed by masked examiners. The primary outcome was change in SER (mean of both eyes) from baseline to 24 months (receiving treatment); other outcomes included change in SER from baseline to 30 months (not receiving treatment) and change in axial length at both time points. Differences were calculated as atropine minus placebo.
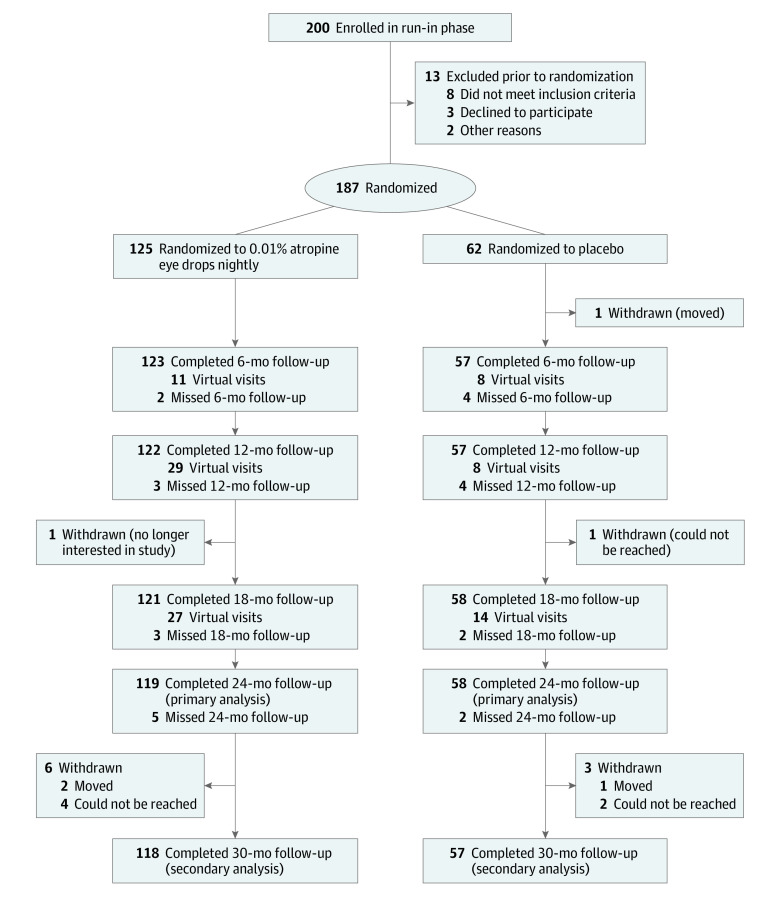
Results: A total of 187 children (mean [SD] age, 10.1 [1.8] years; age range, 5.1-12.9 years; 101 female [54%]; 34 Black [18%], 20 East Asian [11%], 30 Hispanic or Latino [16%], 11 multiracial [6%], 6 West/South Asian [3%], 86 White [46%]) were included in the study. A total of 125 children (67%) received atropine, 0.01%, and 62 children (33%) received placebo. Follow-up was completed at 24 months by 119 of 125 children (95%) in the atropine group and 58 of 62 children (94%) in the placebo group. At 30 months, follow-up was completed by 118 of 125 children (94%) in the atropine group and 57 of 62 children (92%) in the placebo group. At the 24-month primary outcome visit, the adjusted mean (95% CI) change in SER from baseline was -0.82 (-0.96 to -0.68) D and -0.80 (-0.98 to -0.62) D in the atropine and placebo groups, respectively (adjusted difference = -0.02 D; 95% CI, -0.19 to +0.15 D; P = .83). At 30 months (6 months not receiving treatment), the adjusted difference in mean SER change from baseline was -0.04 D (95% CI, -0.25 to +0.17 D). Adjusted mean (95% CI) changes in axial length from baseline to 24 months were 0.44 (0.39-0.50) mm and 0.45 (0.37-0.52) mm in the atropine and placebo groups, respectively (adjusted difference = -0.002 mm; 95% CI, -0.106 to 0.102 mm). Adjusted difference in mean axial elongation from baseline to 30 months was +0.009 mm (95% CI, -0.115 to 0.134 mm).
Conclusions and relevance: In this randomized clinical trial of school-aged children in the US with low to moderate myopia, atropine, 0.01%, eye drops administered nightly when compared with placebo did not slow myopia progression or axial elongation. These results do not support use of atropine, 0.01%, eye drops to slow myopia progression or axial elongation in US children.
Trial registration: ClinicalTrials.gov Identifier: NCT03334253.
Conflict of interest statement
Figures
Comment on
-
Atropine, 0.01%, for Myopia Control.JAMA Ophthalmol. 2023 Aug 1;141(8):766-767. doi: 10.1001/jamaophthalmol.2023.3076. JAMA Ophthalmol. 2023. PMID: 37440252 No abstract available.
References
-
- National Eye Institute . Nearsightedness (myopia) tables. Accessed June 2, 2022. https://www.nei.nih.gov/learn-about-eye-health/eye-health-data-and-stati...
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
