

Clinical and Demographic Factors Associated With COVID-19, Severe COVID-19, and SARS-CoV-2 Infection in Adults: A Secondary Cross-Protocol Analysis of 4 Randomized Clinical Trials
- PMID: 37440227
- PMCID: PMC10346130
- DOI: 10.1001/jamanetworkopen.2023.23349
Clinical and Demographic Factors Associated With COVID-19, Severe COVID-19, and SARS-CoV-2 Infection in Adults: A Secondary Cross-Protocol Analysis of 4 Randomized Clinical Trials
Abstract
Importance: Current data identifying COVID-19 risk factors lack standardized outcomes and insufficiently control for confounders.
Objective: To identify risk factors associated with COVID-19, severe COVID-19, and SARS-CoV-2 infection.
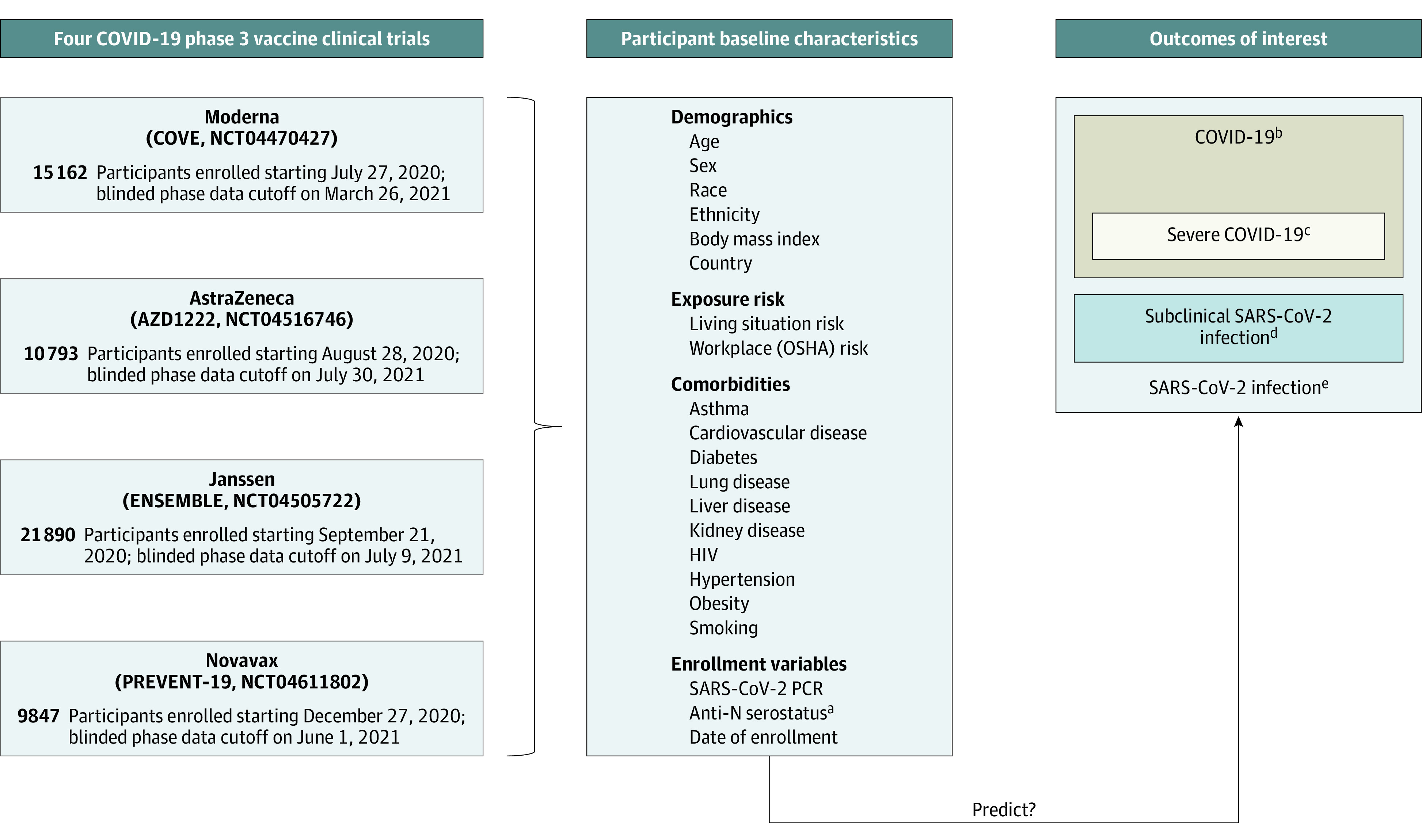
Design, setting, and participants: This secondary cross-protocol analysis included 4 multicenter, international, randomized, blinded, placebo-controlled, COVID-19 vaccine efficacy trials with harmonized protocols established by the COVID-19 Prevention Network. Individual-level data from participants randomized to receive placebo within each trial were combined and analyzed. Enrollment began July 2020 and the last data cutoff was in July 2021. Participants included adults in stable health, at risk for SARS-CoV-2, and assigned to the placebo group within each vaccine trial. Data were analyzed from April 2022 to February 2023.
Exposures: Comorbid conditions, demographic factors, and SARS-CoV-2 exposure risk at the time of enrollment.
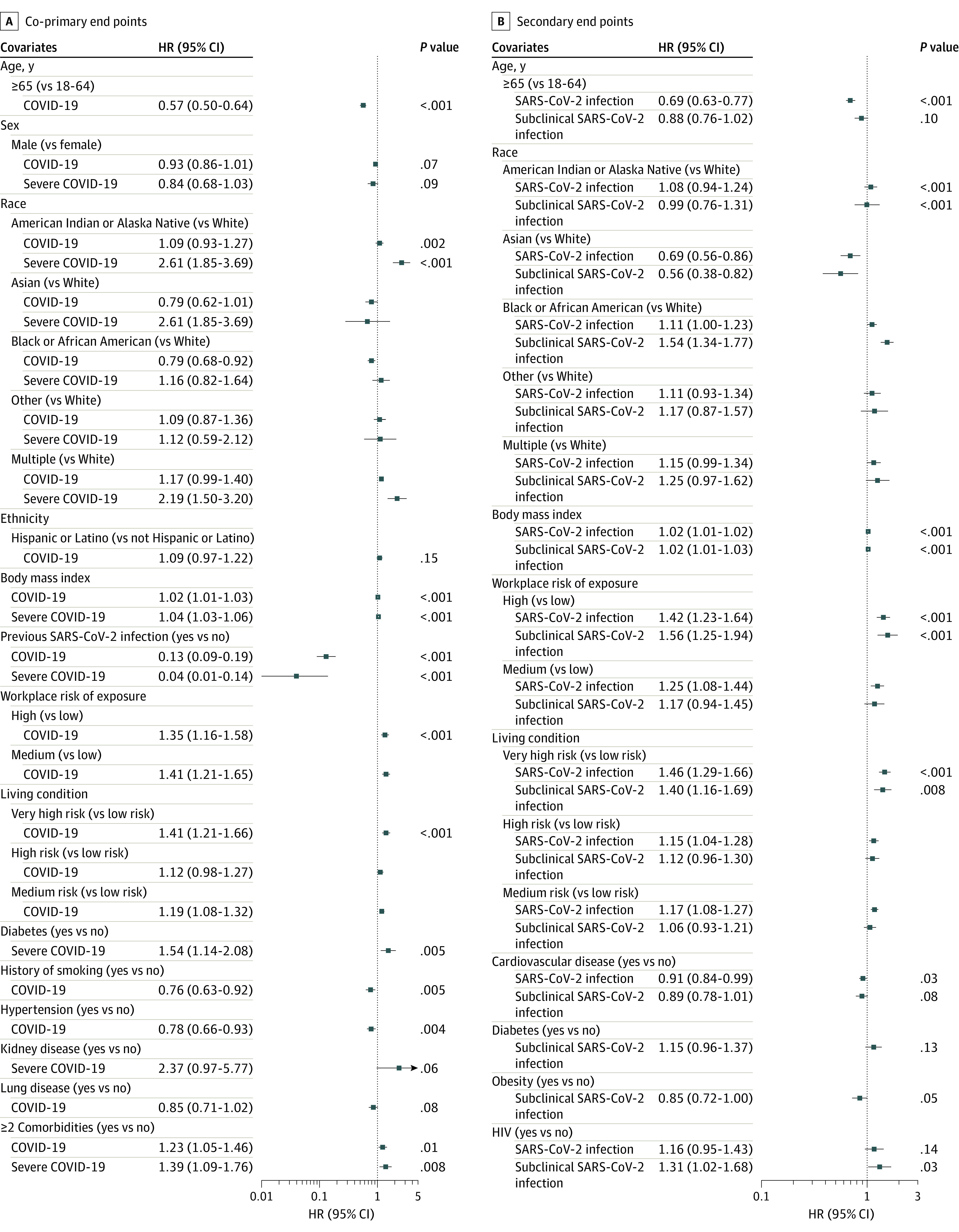
Main outcomes and measures: Coprimary outcomes were COVID-19 and severe COVID-19. Multivariate Cox proportional regression models estimated adjusted hazard ratios (aHRs) and 95% CIs for baseline covariates, accounting for trial, region, and calendar time. Secondary outcomes included severe COVID-19 among people with COVID-19, subclinical SARS-CoV-2 infection, and SARS-CoV-2 infection.
Results: A total of 57 692 participants (median [range] age, 51 [18-95] years; 11 720 participants [20.3%] aged ≥65 years; 31 058 participants [53.8%] assigned male at birth) were included. The analysis population included 3270 American Indian or Alaska Native participants (5.7%), 7849 Black or African American participants (13.6%), 17 678 Hispanic or Latino participants (30.6%), and 40 745 White participants (70.6%). Annualized incidence was 13.9% (95% CI, 13.3%-14.4%) for COVID-19 and 2.0% (95% CI, 1.8%-2.2%) for severe COVID-19. Factors associated with increased rates of COVID-19 included workplace exposure (high vs low: aHR, 1.35 [95% CI, 1.16-1.58]; medium vs low: aHR, 1.41 [95% CI, 1.21-1.65]; P < .001) and living condition risk (very high vs low risk: aHR, 1.41 [95% CI, 1.21-1.66]; medium vs low risk: aHR, 1.19 [95% CI, 1.08-1.32]; P < .001). Factors associated with decreased rates of COVID-19 included previous SARS-CoV-2 infection (aHR, 0.13 [95% CI, 0.09-0.19]; P < .001), age 65 years or older (aHR vs age <65 years, 0.57 [95% CI, 0.50-0.64]; P < .001) and Black or African American race (aHR vs White race, 0.78 [95% CI, 0.67-0.91]; P = .002). Factors associated with increased rates of severe COVID-19 included race (American Indian or Alaska Native vs White: aHR, 2.61 [95% CI, 1.85-3.69]; multiracial vs White: aHR, 2.19 [95% CI, 1.50-3.20]; P < .001), diabetes (aHR, 1.54 [95% CI, 1.14-2.08]; P = .005) and at least 2 comorbidities (aHR vs none, 1.39 [95% CI, 1.09-1.76]; P = .008). In analyses restricted to participants who contracted COVID-19, increased severe COVID-19 rates were associated with age 65 years or older (aHR vs <65 years, 1.75 [95% CI, 1.32-2.31]; P < .001), race (American Indian or Alaska Native vs White: aHR, 1.98 [95% CI, 1.38-2.83]; Black or African American vs White: aHR, 1.49 [95% CI, 1.03-2.14]; multiracial: aHR, 1.81 [95% CI, 1.21-2.69]; overall P = .001), body mass index (aHR per 1-unit increase, 1.03 [95% CI, 1.01-1.04]; P = .001), and diabetes (aHR, 1.85 [95% CI, 1.37-2.49]; P < .001). Previous SARS-CoV-2 infection was associated with decreased severe COVID-19 rates (aHR, 0.04 [95% CI, 0.01-0.14]; P < .001).
Conclusions and relevance: In this secondary cross-protocol analysis of 4 randomized clinical trials, exposure and demographic factors had the strongest associations with outcomes; results could inform mitigation strategies for SARS-CoV-2 and viruses with comparable epidemiological characteristics.
Conflict of interest statement
Figures


Comment in
-
COVID-19 Vaccine Placebo Group Analyses.JAMA Netw Open. 2023 Jul 3;6(7):e2323316. doi: 10.1001/jamanetworkopen.2023.23316. JAMA Netw Open. 2023. PMID: 37440235 No abstract available.
References
-
- World Health Organization . Weekly operational update on COVID-19. Accessed June 6, 2023. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situatio...
-
- Johns Hopkins Coronavirus Research Center . Accessed June 6, 2023. https://coronavirus.jhu.edu/
-
- Kilpatrick RD, Sánchez-Soliño O, Alami NN, et al. . Epidemiological Population Study of SARS-CoV-2 in Lake County, Illinois (CONTACT): methodology and baseline characteristics of a community-based surveillance study. Infect Dis Ther. 2022;11(2):899-911. doi:10.1007/s40121-022-00593-0 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UM1 AI069494/AI/NIAID NIH HHS/United States
- U01 AI069470/AI/NIAID NIH HHS/United States
- I01 BX000207/BX/BLRD VA/United States
- UM1 AI069534/AI/NIAID NIH HHS/United States
- UM1 AI148685/AI/NIAID NIH HHS/United States
- UM1 AI069481/AI/NIAID NIH HHS/United States
- UM1 AI068614/AI/NIAID NIH HHS/United States
- UM1 AI154468/AI/NIAID NIH HHS/United States
- UM1 AI148689/AI/NIAID NIH HHS/United States
- UM1 AI148450/AI/NIAID NIH HHS/United States
- UM1 AI069476/AI/NIAID NIH HHS/United States
- UM1 AI069424/AI/NIAID NIH HHS/United States
- UM1 AI148575/AI/NIAID NIH HHS/United States
- U01 AI069476/AI/NIAID NIH HHS/United States
- UM1 AI148576/AI/NIAID NIH HHS/United States
- P30 AI045008/AI/NIAID NIH HHS/United States
- UM1 AI069412/AI/NIAID NIH HHS/United States
- UM1 AI069470/AI/NIAID NIH HHS/United States
- UL1 TR002378/TR/NCATS NIH HHS/United States
- UM1 AI068635/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
