

Sex differences in pediatric caudal epidural anesthesia under sedation without primary airway instrumentation
- PMID: 37440538
- PMCID: PMC10343088
- DOI: 10.1371/journal.pone.0288431
Sex differences in pediatric caudal epidural anesthesia under sedation without primary airway instrumentation
Abstract
Study objective: To identify sex differences associated with caudal epidurals, the most commonly used technique of pediatric regional anesthesia, based on individually validated data of ultrasound-guided blocks performed between 04/2014 and 12/2020.
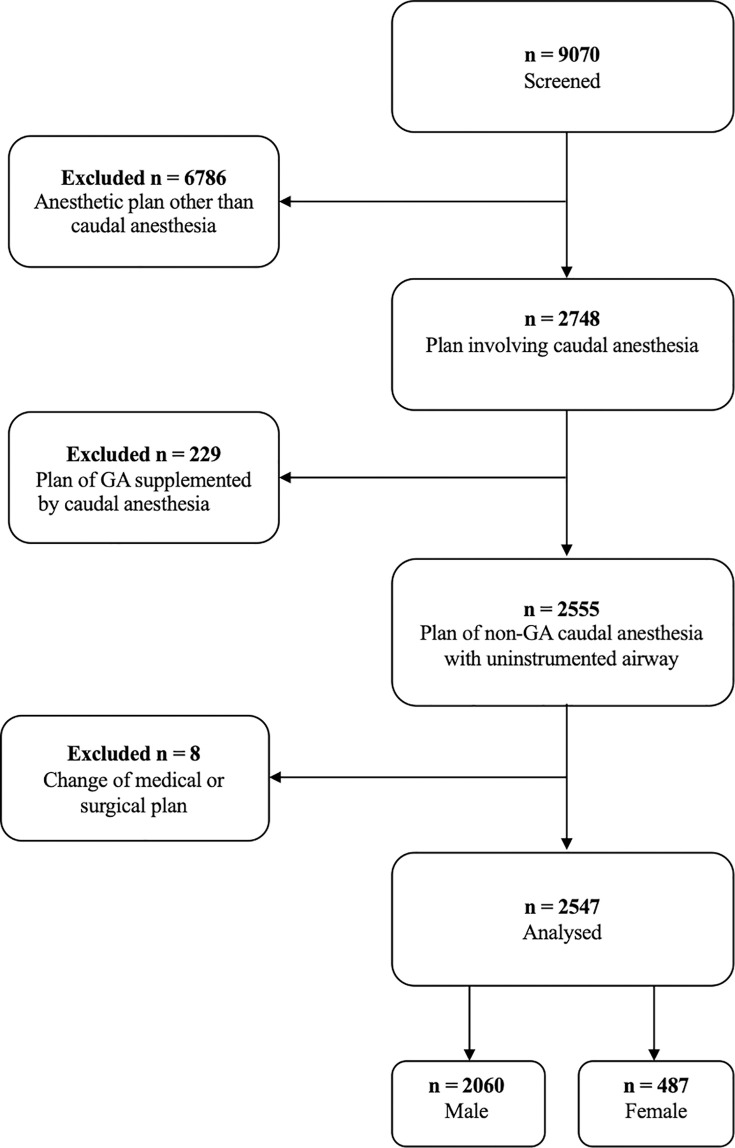
Methods: Prospectively collected and individually validated data of a cohort of children aged between 0-15 years was analyzed in a retrospective observational study. We included pediatric surgeries involving a primary plan of caudal epidural anesthesia under sedation (without airway instrumentation) and a contingency plan of general anesthesia. Sex-specific rates were analyzed for overall failure of the primary anesthesia plan, for residual pain, for block-related technical complications and for critical respiratory events. We used Fisher´s exact tests and multivariable logistic regressions were used to evaluate sex-specific associations.
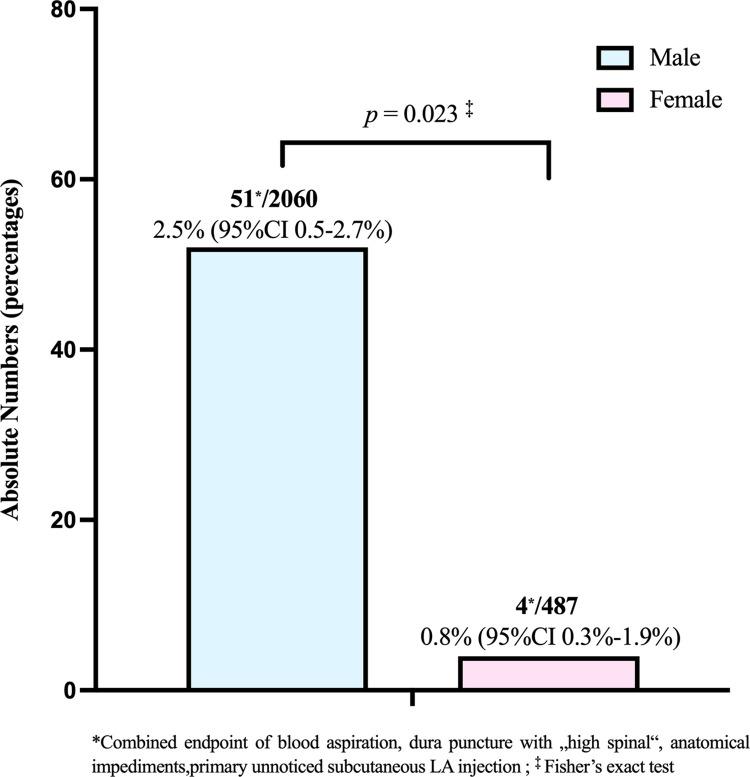
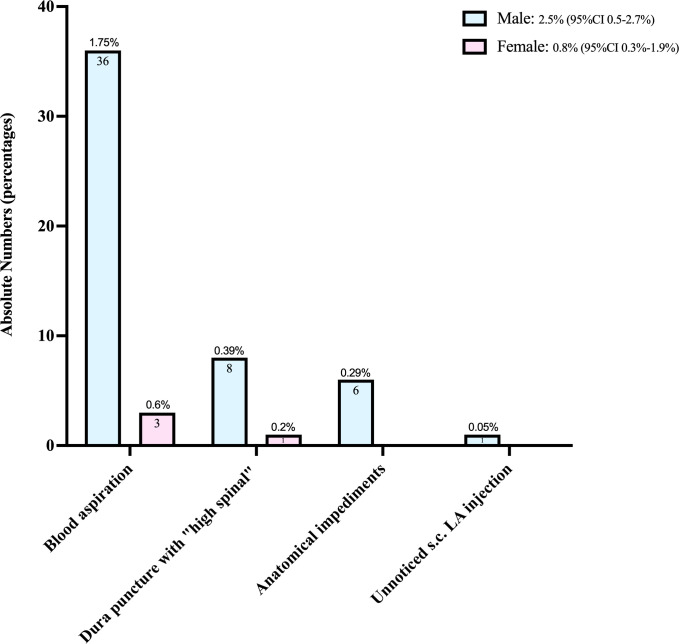
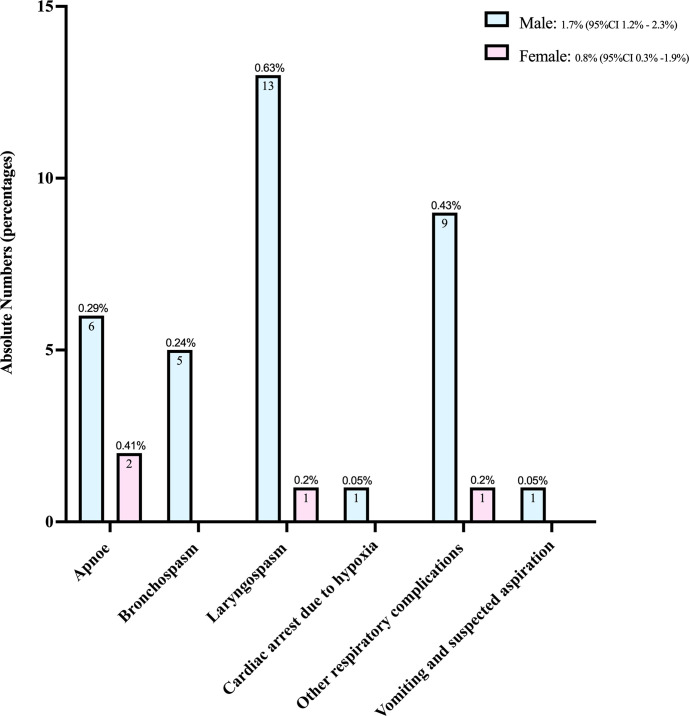
Results: Data from 487 girls and 2060 boys ≤15 years old (ASA status 1 to 4) were analyzed. The primary-anesthesia-plan failure rate was 5.5% (95%CI 3.8%-7.8%) (N = 27/487) among girls and 4.7% (95%CI 3.9%-5.7%) (N = 97/2060) among boys (p = 0.41). Residual pain was the main cause of failure, with rates of 4.5% (95%CI 2.9-6.6%) (N = 22/487) among girls and 3.0% (95%CI 2.3-3.8%) (N = 61/2060) among boys (p = 0.089). Block-related technical complications were seen at rates of 0.8% (95%CI 0.3%-1.9%) (N = 4/487) among girls vs 2.5% (95%CI 0.5-2.7%) (N = 51/2060) among boys and, hence, significantly more often among male patients (p = 0.023). Male sex was significantly associated with higher odds (adjusted OR: 3.18; 95% CI: 1.12-9; p = 0.029) for such technical complications regardless of age, ASA status, gestational week at birth or puncture attempts. Critical respiratory events occurred at a 1.7% (95%CI 1.2%-2.3%) rate (N = 35/2060) twice as high among boys as 0.8% (95%CI 0.3%-1.9%) (N = 4/487) among girls (p = 0.21).
Conclusions: While the the primary-anesthesia-plan failure rate was equal for girls and boys, technical complications and respiratory events are more likely to occur in boys.
Copyright: © 2023 Opfermann et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Ultrasound-guided caudal blockade and sedation for paediatric surgery: a retrospective cohort study.Anaesthesia. 2022 Jul;77(7):785-794. doi: 10.1111/anae.15738. Epub 2022 Apr 22. Anaesthesia. 2022. PMID: 35460068 Free PMC article.
-
Combined spinal/caudal catheter anesthesia: extending the boundaries of regional anesthesia for complex pediatric urological surgery.J Pediatr Urol. 2019 Oct;15(5):442-447. doi: 10.1016/j.jpurol.2019.04.004. Epub 2019 Apr 11. J Pediatr Urol. 2019. PMID: 31085139
-
Regional anesthesia is a good alternative to general anesthesia in pediatric surgery: Experience in 1,554 children.J Pediatr Surg. 2002 Apr;37(4):610-3. doi: 10.1053/jpsu.2002.31619. J Pediatr Surg. 2002. PMID: 11912520
-
[Caudal Anesthesia: Overview and Practical Recommendations].Anasthesiol Intensivmed Notfallmed Schmerzther. 2022 Nov;57(11-12):724-736. doi: 10.1055/a-1467-8624. Epub 2022 Nov 29. Anasthesiol Intensivmed Notfallmed Schmerzther. 2022. PMID: 36446359 Review. German.
-
Awake caudals and epidurals should be used more frequently in neonates and infants.Paediatr Anaesth. 2015 Jan;25(1):93-9. doi: 10.1111/pan.12543. Epub 2014 Sep 30. Paediatr Anaesth. 2015. PMID: 25265914 Review.
Cited by
-
Anesthetic outcomes in pediatric tonsillectomy: insights from the Palestinian experience.Perioper Med (Lond). 2025 May 9;14(1):54. doi: 10.1186/s13741-025-00537-5. Perioper Med (Lond). 2025. PMID: 40346655 Free PMC article.
References
-
- Cabrera OH, Gulvezan T, Symmes B, Quillinan N, Jevtovic-Todorovic V. Sex differences in neurodevelopmental abnormalities caused by early-life anaesthesia exposure: a narrative review. Br J Anaesth. 2020;124(3):e81–e91. Epub 2020/01/26. doi: 10.1016/j.bja.2019.12.032 ; PubMed Central PMCID: PMC7050624. - DOI - PMC - PubMed
-
- Geller SE, Koch AR, Roesch P, Filut A, Hallgren E, Carnes M. The More Things Change, the More They Stay the Same: A Study to Evaluate Compliance With Inclusion and Assessment of Women and Minorities in Randomized Controlled Trials. Acad Med. 2018;93(4):630–5. doi: 10.1097/ACM.0000000000002027 ; PubMed Central PMCID: PMC5908758. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
