

The Role of Serum and Peritoneal Biomarkers in Predicting Sepsis and Septic Multiorgan Failure in Patients With Secondary Peritonitis
- PMID: 37441100
- PMCID: PMC10335813
- DOI: 10.7759/cureus.41724
The Role of Serum and Peritoneal Biomarkers in Predicting Sepsis and Septic Multiorgan Failure in Patients With Secondary Peritonitis
Abstract
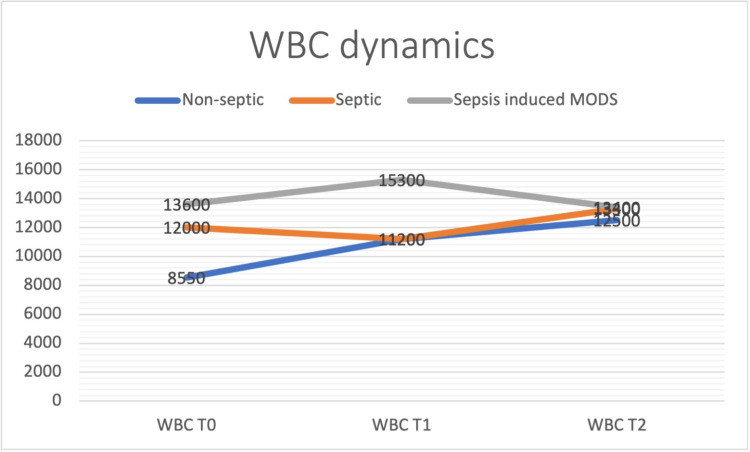
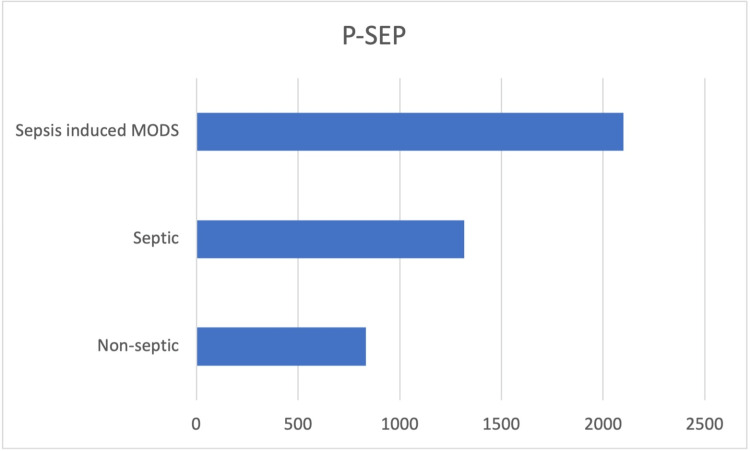
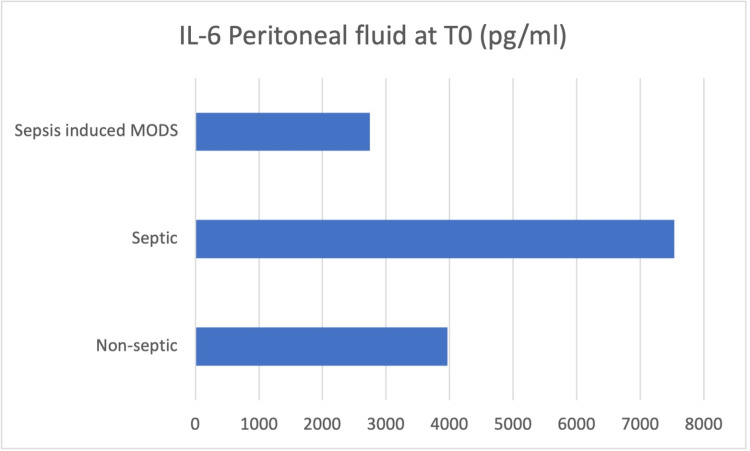
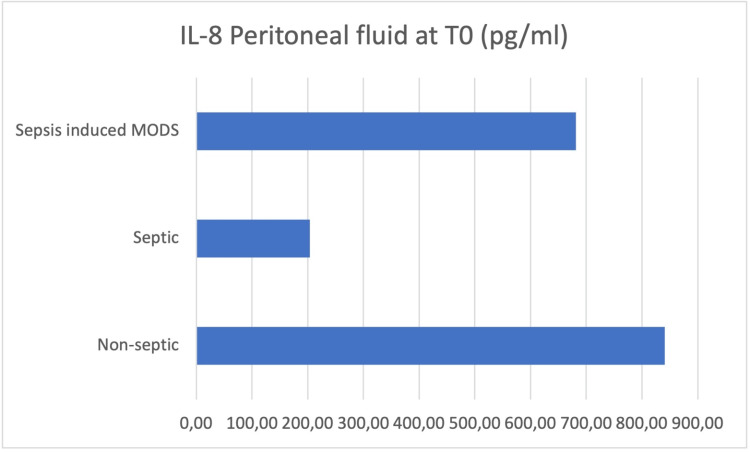
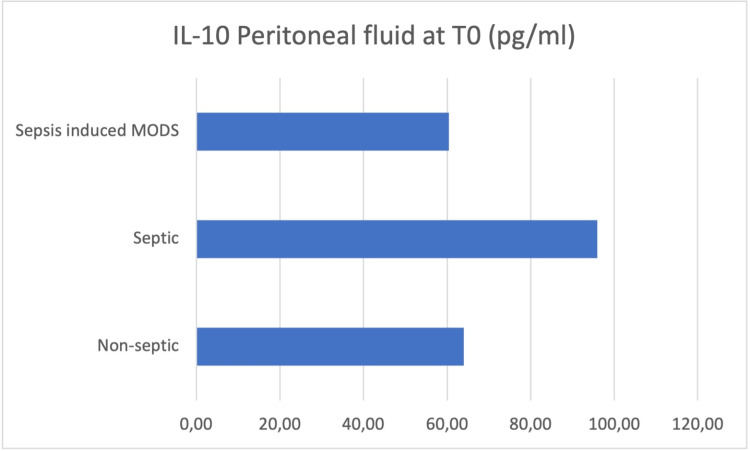
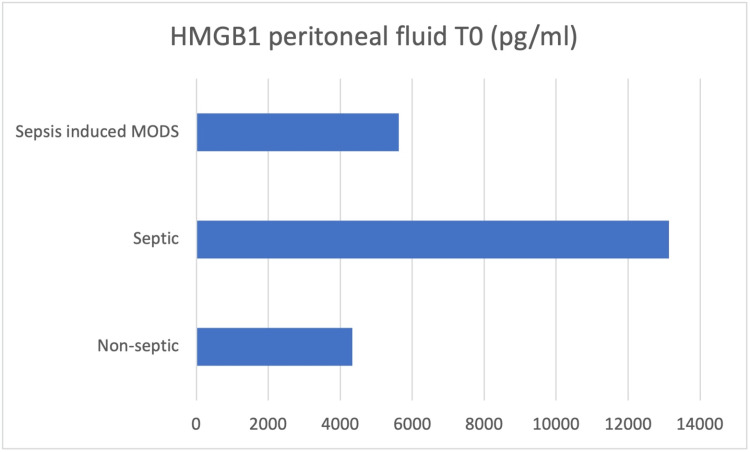
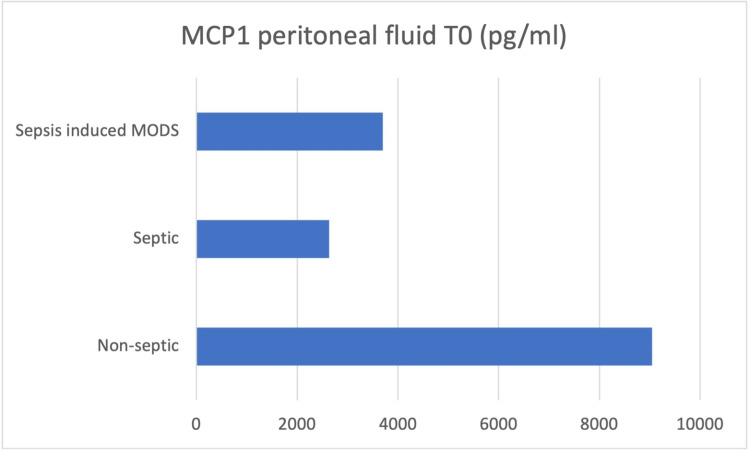
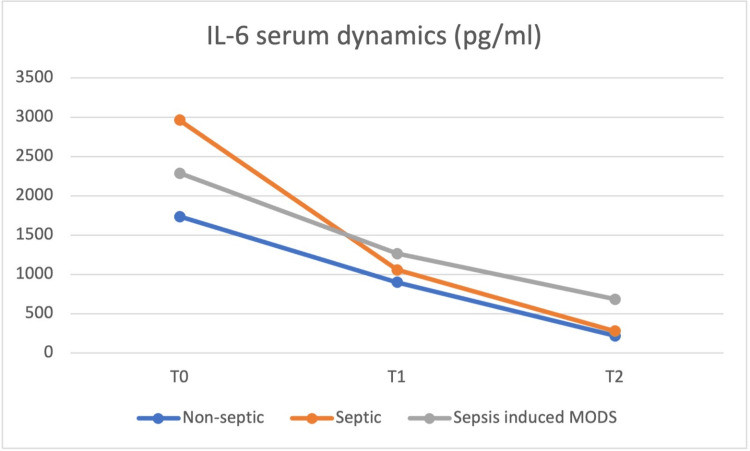
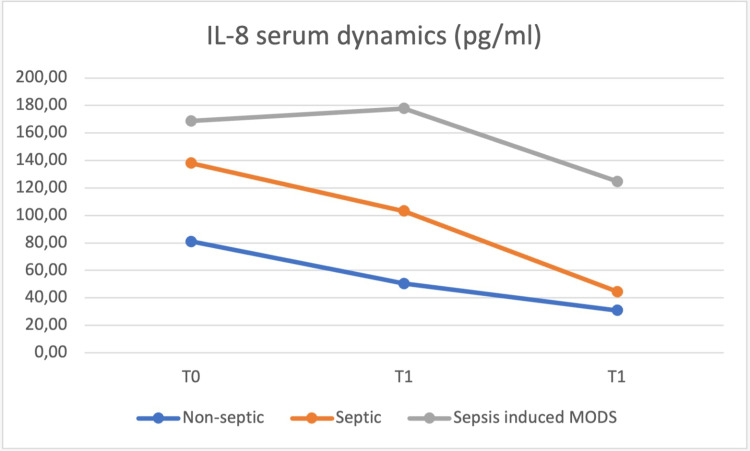
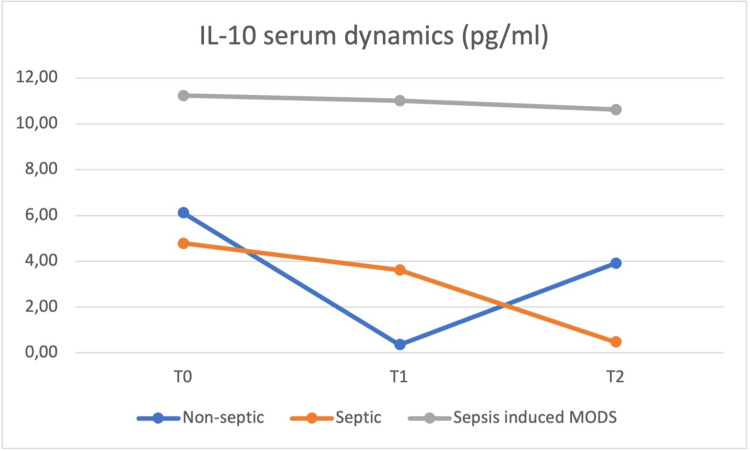
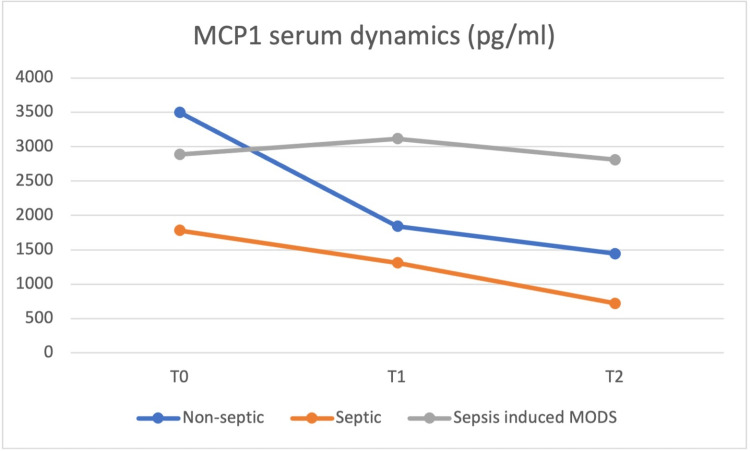
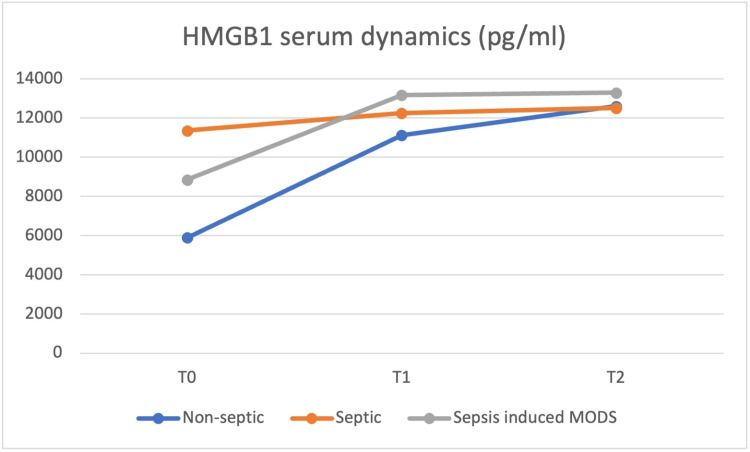
Purpose Secondary peritonitis is still one of the most important causes of severe sepsis in the world; therefore, it is of utmost importance to identify biomarkers that could be employed for the purpose of selecting patients at high risk for developing life-threatening complications after emergency surgery. In view of this quest, our study seeks to reveal the possible role for serum and peritoneal concentrations of selected biomarkers, specifically presepsin, procalcitonin, monocyte chemoattractant protein-1 (MCP-1), high mobility group box 1 protein (HMGB-1) and interleukins (IL-6, -8, -10), in early prediction of sepsis and septic multiorgan failure for patients with secondary peritonitis. Methods We prospectively observed 32 selected patients with secondary peritonitis that underwent emergency surgery. Blood and peritoneal fluid samples were drawn at the time of surgery (T0), and after that, blood samples were taken at 24 (T1) and 48 (T2) hours postoperatively. Cytokines concentrations were determined using a sandwich enzyme-linked immunosorbent assay (ELISA), a non-competitive variant, both in peritoneal fluid and serum. For determining whole blood concentration of presepsin and procalcitonin, PATHFAST™ assays (Polymedco, Cortlandt, New York) were used, based on the principle of non-competitive chemiluminescent enzyme immune-assay (CLEIA). The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of University Emergency Hospital Bucharest (no. 40325/6 April 2023). Results We found significant elevations in the peritoneal concentrations of interleukins 6, 8, 10, HMGB-1, and MCP-1 in all patients with secondary peritonitis at the moment of surgery; however, no clear correlation could be made based on this data with patient evolution. With regards to blood concentrations of the aforementioned serum cytokines and presepsin, procalcitonin (as already established markers of sepsis), our results showed good predictive value of presepsin for developing sepsis and septic multiorgan failure from the first hours in this patient category. All other biomarkers, despite having higher concentrations than baseline, in particular at 24-48 hours after surgery, had unpredictable dynamics that couldn't be correlated with the severity of the disease. Conclusion Cytokine production is the mainstay in developing sepsis and septic multiorgan failure in patients with secondary peritonitis; therefore, studying the dynamics of said cytokines seems of interest in finding tools to predict the development of sepsis or sepsis-related mortality. However, at the time, there seemed to be no clear correlation between the values of these cytokines and the development of complications.
Keywords: cytokine storm; peritoneal cytokines; secondary peritonitis; sepsis; syndrome.
Copyright © 2023, Dumitrascu et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Predictive Role of Changes in Presepsin and Early Sepsis in ICU Patients After Abdominal Surgery.J Surg Res. 2022 Oct;278:207-215. doi: 10.1016/j.jss.2022.04.072. Epub 2022 May 24. J Surg Res. 2022. PMID: 35623266
-
Evaluation of Biomarkers from Peritoneal Fluid as Predictors of Severity for Abdominal Sepsis Patients Following Emergency Laparotomy.J Inflamm Res. 2023 Feb 24;16:809-826. doi: 10.2147/JIR.S401428. eCollection 2023. J Inflamm Res. 2023. PMID: 36876154 Free PMC article.
-
Evaluation of procalcitonin for predicting septic multiorgan failure and overall prognosis in secondary peritonitis: a prospective, international multicenter study.Arch Surg. 2007 Feb;142(2):134-42. doi: 10.1001/archsurg.142.2.134. Arch Surg. 2007. PMID: 17309964
-
The efficacy of procalcitonin as a biomarker in the management of sepsis: slaying dragons or tilting at windmills?Surg Infect (Larchmt). 2013 Dec;14(6):489-511. doi: 10.1089/sur.2012.028. Epub 2013 Nov 25. Surg Infect (Larchmt). 2013. PMID: 24274059 Review.
-
Presepsin as a Diagnostic and Prognostic Biomarker in Sepsis.Cureus. 2021 May 13;13(5):e15019. doi: 10.7759/cureus.15019. Cureus. 2021. PMID: 34150378 Free PMC article. Review.
Cited by
-
Procalcitonin and interleukin- 6 in predicting prognosis of sepsis patients with cancer.Support Care Cancer. 2025 Apr 22;33(5):404. doi: 10.1007/s00520-025-09464-z. Support Care Cancer. 2025. PMID: 40261444
-
Early Fever in Allogeneic Stem Cell Transplantation: Are Presepsin and YKL-40 Valuable Diagnostic Tools?J Clin Med. 2024 Oct 8;13(19):5991. doi: 10.3390/jcm13195991. J Clin Med. 2024. PMID: 39408051 Free PMC article.
References
-
- Secondary peritonitis and intra-abdominal sepsis: an increasingly global disease in search of better systemic therapies. Clements TW, Tolonen M, Ball CG, Kirkpatrick AW. Scand J Surg. 2021;110:139–149. - PubMed
-
- Procalcitonin: improved biochemical severity stratification and postoperative monitoring in severe abdominal inflammation and sepsis. Rau B, Krüger CM, Schilling MK. Langenbecks Arch Surg. 2004;389:134–144. - PubMed
-
- Mechanical safety study and antibiotic‑loaded polymethylmethacrylate spacers threshold, manufactured intraoperatively in orthopaedic surgery. Cursaru A, Cretu B, Serban B, et al. MaterPlast. 1964;57:317.
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous