

Oxidised IL-33 drives COPD epithelial pathogenesis via ST2-independent RAGE/EGFR signalling complex
- PMID: 37442582
- PMCID: PMC10533947
- DOI: 10.1183/13993003.02210-2022
Oxidised IL-33 drives COPD epithelial pathogenesis via ST2-independent RAGE/EGFR signalling complex
Abstract
Background: Epithelial damage, repair and remodelling are critical features of chronic airway diseases including chronic obstructive pulmonary disease (COPD). Interleukin (IL)-33 released from damaged airway epithelia causes inflammation via its receptor, serum stimulation-2 (ST2). Oxidation of IL-33 to a non-ST2-binding form (IL-33ox) is thought to limit its activity. We investigated whether IL-33ox has functional activities that are independent of ST2 in the airway epithelium.
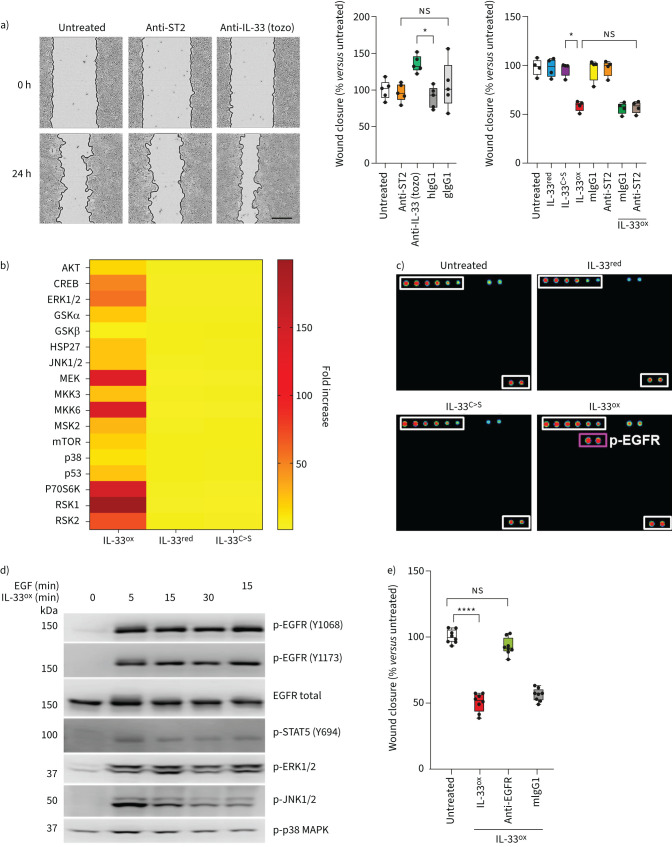
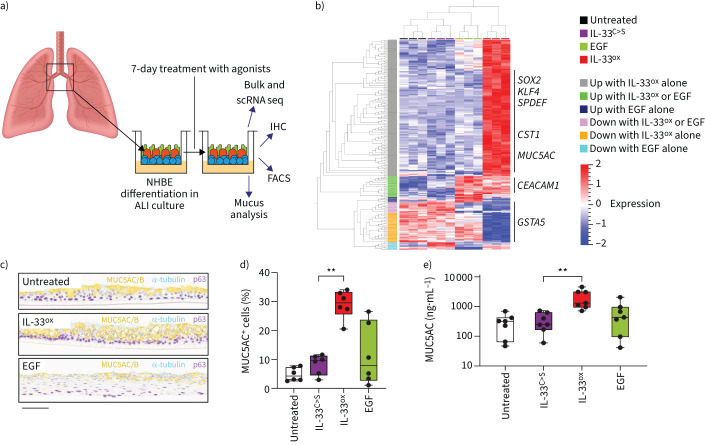
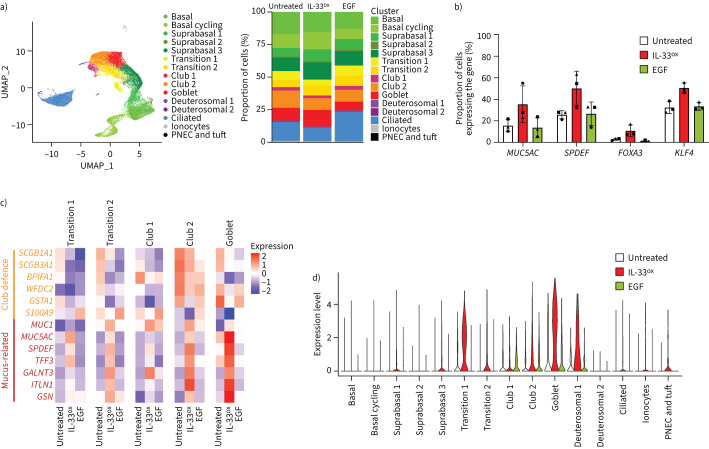
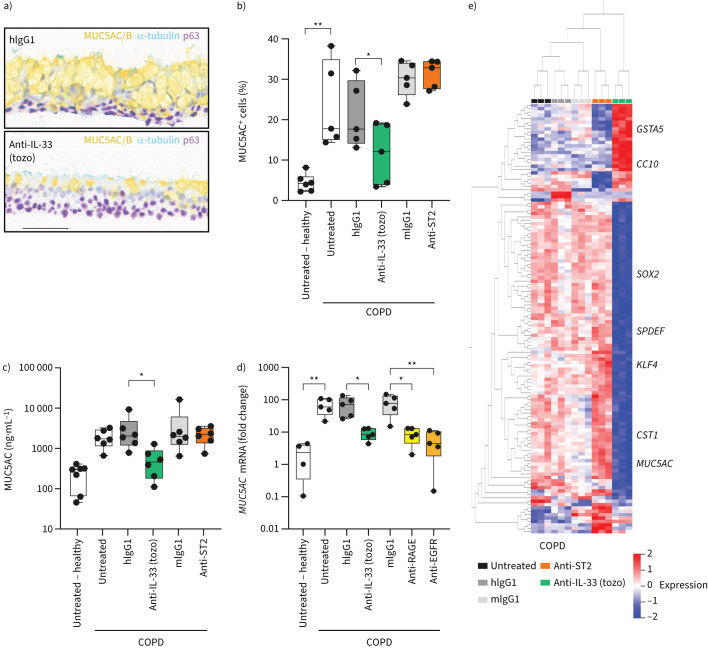
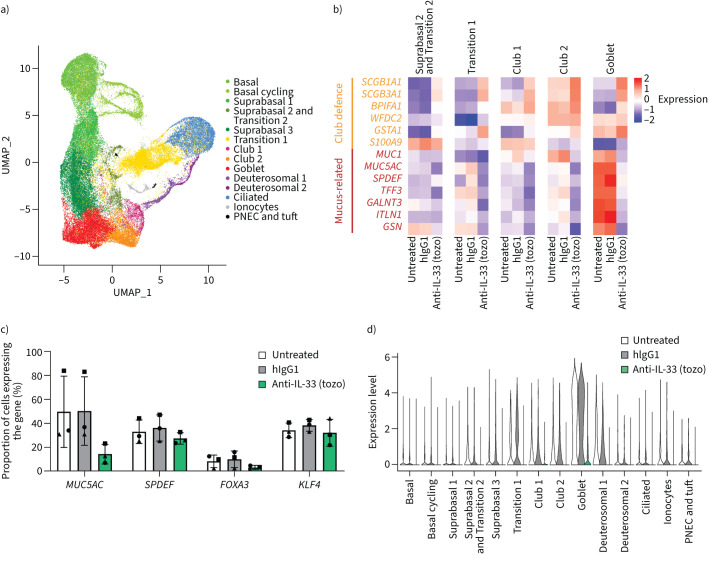
Methods: In vitro epithelial damage assays and three-dimensional, air-liquid interface (ALI) cell culture models of healthy and COPD epithelia were used to elucidate the functional role of IL-33ox. Transcriptomic changes occurring in healthy ALI cultures treated with IL-33ox and COPD ALI cultures treated with an IL-33-neutralising antibody were assessed with bulk and single-cell RNA sequencing analysis.
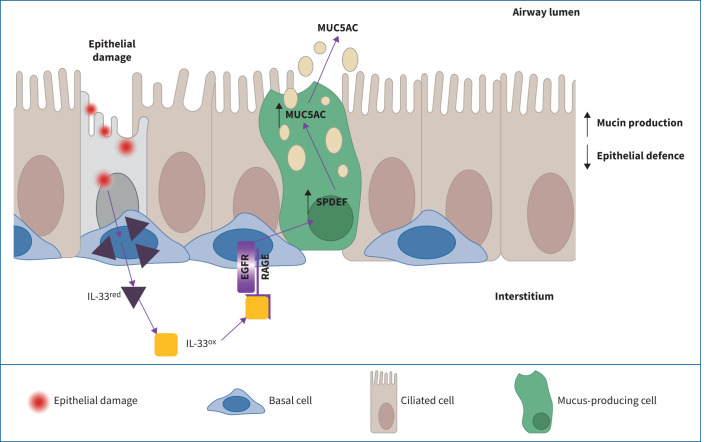
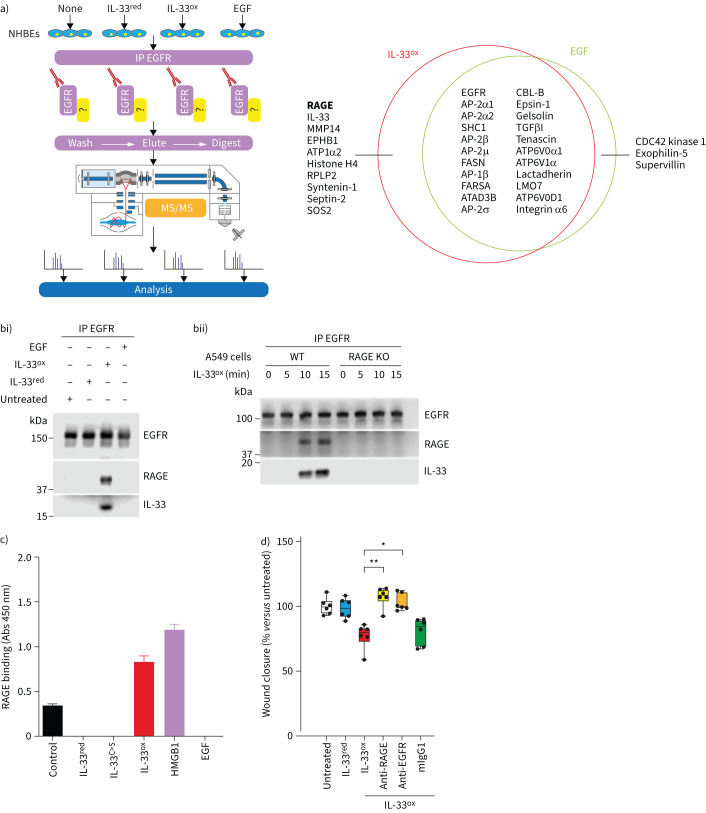
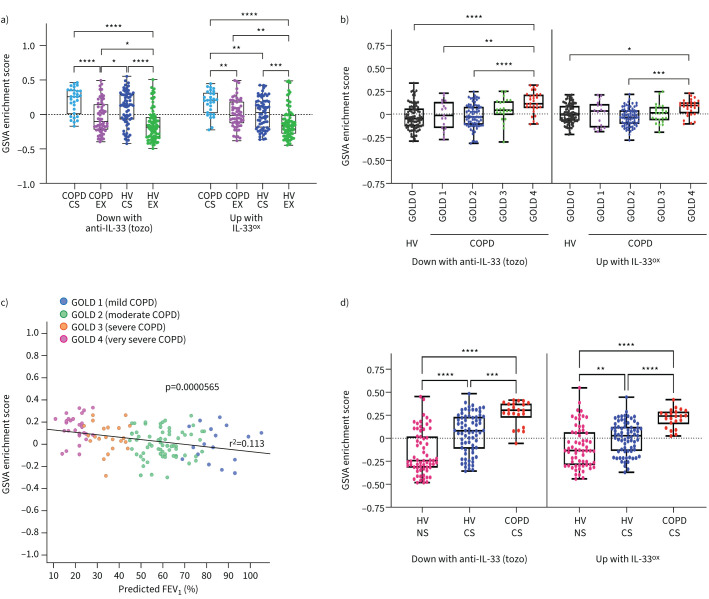
Results: We demonstrate that IL-33ox forms a complex with receptor for advanced glycation end products (RAGE) and epidermal growth factor receptor (EGFR) expressed on airway epithelium. Activation of this alternative, ST2-independent pathway impaired epithelial wound closure and induced airway epithelial remodelling in vitro. IL-33ox increased the proportion of mucus-producing cells and reduced epithelial defence functions, mimicking pathogenic traits of COPD. Neutralisation of the IL-33ox pathway reversed these deleterious traits in COPD epithelia. Gene signatures defining the pathogenic effects of IL-33ox were enriched in airway epithelia from patients with severe COPD.
Conclusions: Our study reveals for the first time that IL-33, RAGE and EGFR act together in an ST2-independent pathway in the airway epithelium and govern abnormal epithelial remodelling and muco-obstructive features in COPD.
Copyright ©The authors 2023.
Conflict of interest statement
Conflict of interest: S. Strickson, V.A. Negri, Y. Ohne, T. Ottosson, R.B. Dodd, C.C. Huntington, T. Baker, J. Li, K.E. Stephenson, A.J. O'Connor, J.S. Sagawe, H. Killick, D.G. Rees, S. Koch, Y. Wang, M. Ghaedi, S. Saumyaa, G.P. Sims, I.C. Scott, X. Romero Ros and E.S. Cohen are employees of AstraZeneca and may hold stock or stock options in AstraZeneca. K.F. Houslay, T. Moore, E. Gubbins, R. Kolbeck and A.A. Humbles are former employees of AstraZeneca and may hold stock or stock options in AstraZeneca. C. Sanden has nothing to disclose. J.S. Erjefält is a founder and board member of Medetect AB.
Figures
Comment in
-
Oxidation alters IL-33 function: new insights in the biology of different forms of IL-33 and their relevance for COPD.Eur Respir J. 2023 Sep 28;62(3):2301301. doi: 10.1183/13993003.01301-2023. Print 2023 Sep. Eur Respir J. 2023. PMID: 37770091 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous