

Different Methods of Minimally Invasive Esophagojejunostomy After Total Gastrectomy for Gastric Cancer: Outcomes from Two Experienced Centers
- PMID: 37442910
- PMCID: PMC10506935
- DOI: 10.1245/s10434-023-13771-2
Different Methods of Minimally Invasive Esophagojejunostomy After Total Gastrectomy for Gastric Cancer: Outcomes from Two Experienced Centers
Abstract
Background: Esophagojejunostomy after minimally invasive total gastrectomy (MITG) for gastric cancer (GC) is technically challenging. Failure of the esophagojejunal anastomosis can lead to significant morbidity, leading to short- and long-term quality of life (QoL) impairment or mortality. The optimal reconstruction method following MITG remains controversial. We evaluated outcomes of minimally invasive esophagojejunostomy after laparoscopic or robotic total gastrectomies.
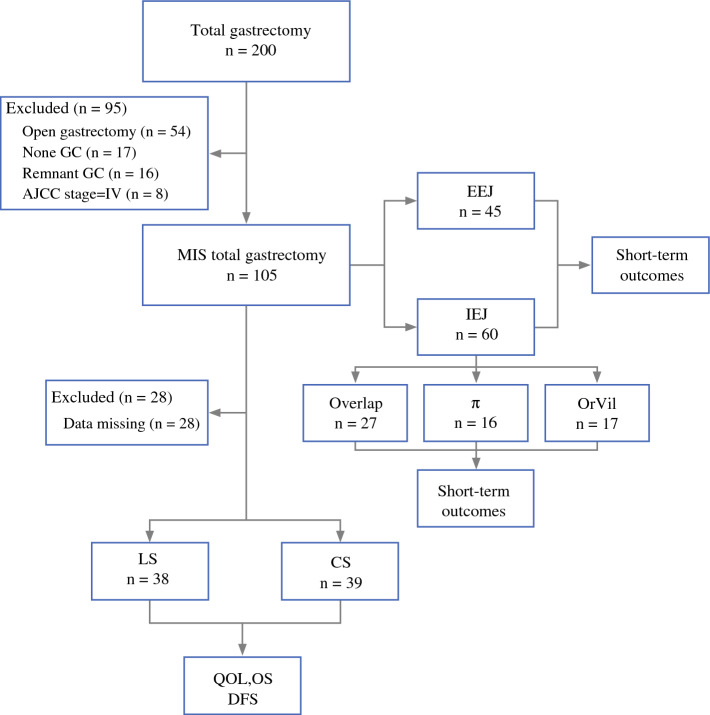
Methods: We retrospectively reviewed MITG patients between 2015 and 2020 at two high-volume centers in China and the United States. Eligible patients were divided into groups by different reconstruction methods. We compared clinicopathologic characteristics, postoperative outcomes, including complication rates, overall survival rate (OS), disease-free survival rate (DFS), and patient-reported QoL.
Results: GC patients (n = 105) were divided into intracorporeal esophagojejunostomy (IEJ, n = 60) and extracorporeal esophagojejunostomy (EEJ, n = 45) groups. EEJ had higher incidence of wound infection (8.3% vs 13.3%, P = 0.044) and pneumonia (21.7% vs 40.0%, P = 0.042) than IEJ. The linear stapler (LS) group was inferior to the circular stapler (CS) group in reflux [50.0 (11.1-77.8) vs 44.4 (0.0-66.7), P = 0.041] and diarrhea [33.3 (0.0-66.7) vs 0.0 (0.0-66.7), P = 0.045] while LS was better than CS for dysphagia [22.2 (0.0-33.3) vs 11.1 (0.0-33.3), P = 0.049] and eating restrictions [33.3 (16.7-58.3) vs 41.7 (16.7-66.7), P = 0.029] at 1 year. OS and DFS did not differ significantly between LS and CS.
Conclusions: IEJ anastomosis generated better results than EEJ. LS was associated with a better patient eating experience, but more diarrhea and reflux compared with CS. Clinical and patient-reported outcomes show the superiority of IEJ with the LS reconstruction method in MITG for GC.
Keywords: Esophagojejunal reconstruction; Esophagojejunostomy; Gastric cancer; Intracorporeal esophagojejunostomy; Minimally invasive total gastrectomy; Quality-of-life.
© 2023. The Author(s).
Conflict of interest statement
Outside the submitted work
Figures


Comment in
-
Editorial: Different Methods of Minimally Invasive Esophagojejunostomy After Total Gastrectomy for Gastric Cancer: Outcomes from Two Experienced Centers.Ann Surg Oncol. 2023 Oct;30(11):6316-6317. doi: 10.1245/s10434-023-13858-w. Epub 2023 Aug 12. Ann Surg Oncol. 2023. PMID: 37573281 No abstract available.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
