

Analgesic effectiveness of serratus anterior plane block in patients undergoing video-assisted thoracoscopic surgery: a systematic review and updated meta-analysis of randomized controlled trials
- PMID: 37442948
- PMCID: PMC10339549
- DOI: 10.1186/s12871-023-02197-8
Analgesic effectiveness of serratus anterior plane block in patients undergoing video-assisted thoracoscopic surgery: a systematic review and updated meta-analysis of randomized controlled trials
Abstract
Background: Serratus anterior plane block (SAPB) is a promising regional technique for analgesia in thoracic surgery. Till now, several randomized controlled trials (RCTs) have explored the effectiveness of SAPB for postoperative pain control in patients undergoing video-assisted thoracoscopic surgery (VATS), but the sample sizes were small and conclusions remained in controversy. Therefore, we conducted the present systematic review and meta-analysis.
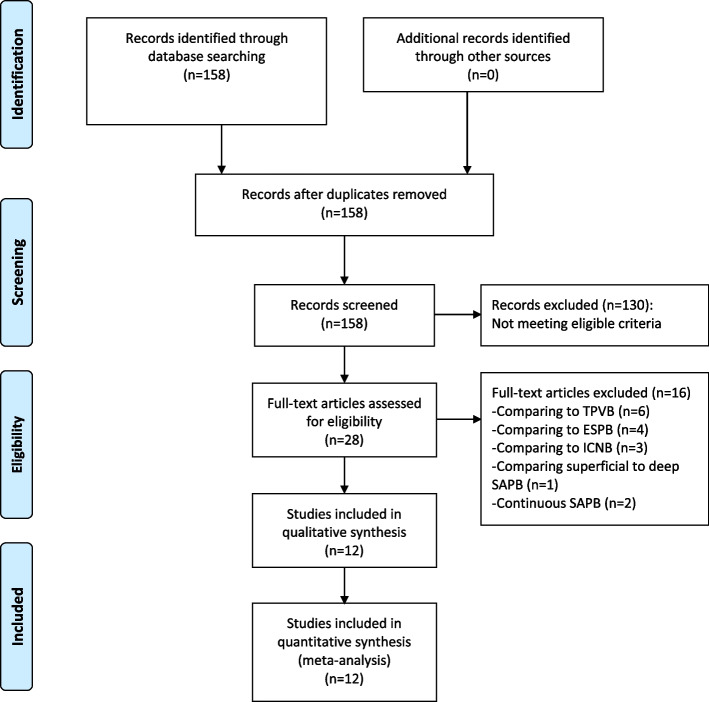
Methods: RCTs evaluating the analgesic performance of SAPB, comparing to control methods (no block, placebo or local infiltration anesthesia), in patients undergoing VATS were searched in PubMed, EMBASE, Web of Science and Cochrane Library from inception to December 31, 2022. Mean difference (MD) and corresponding 95% confidence interval (95%CI) were calculated for postoperative pain scores at various time points, postoperative opioid consumption and length of hospital stay. Pooled relative risk (RR) with 95%CI were calculated for the risk of postoperative nausea and vomiting (PONV) and dizziness. A random-effect model was applied.
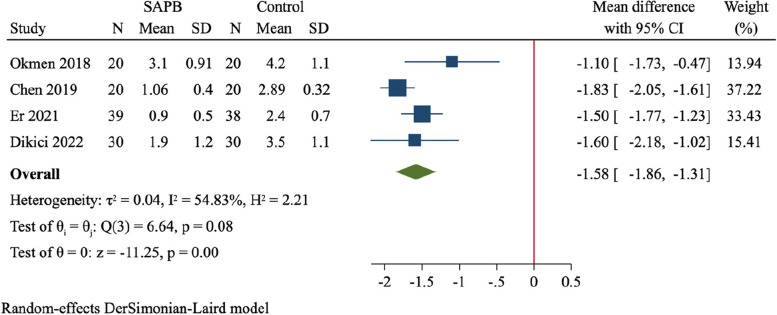
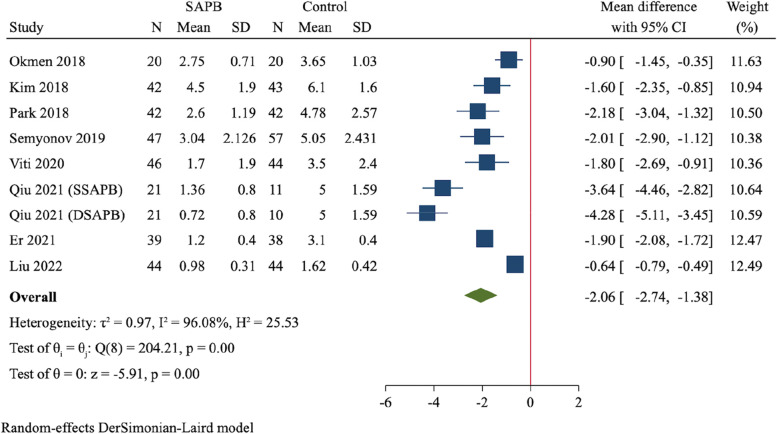
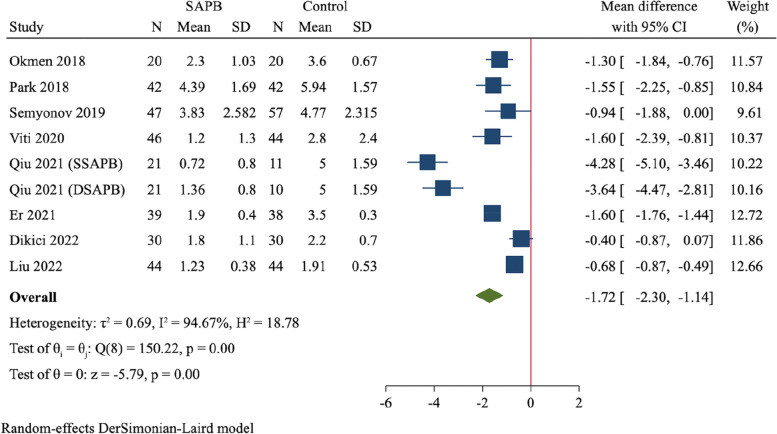
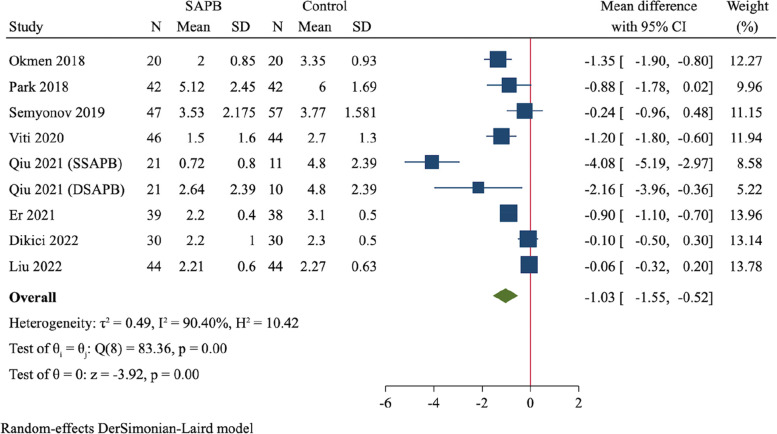
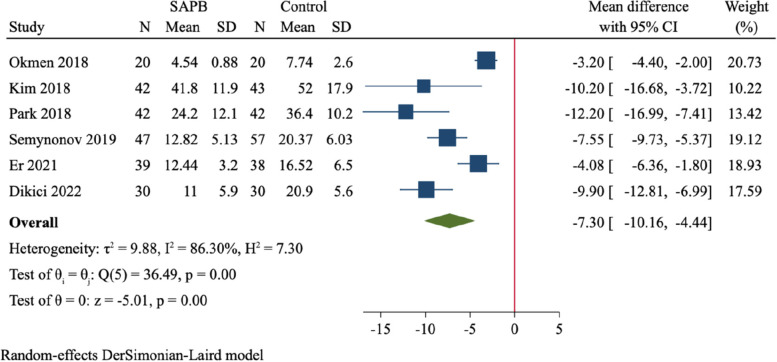
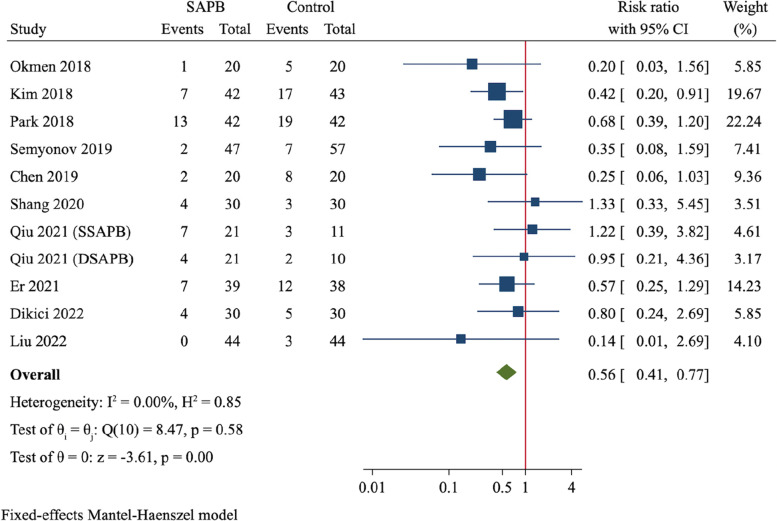
Results: A total of 12 RCTs (837 participants) were finally included. Compared to control group, SAPB had significant reductions of postoperative pain scores at 2 h (MD = -1.58, 95%CI: -1.86 to -1.31, P < 0.001), 6 h (MD = -2.06, 95%CI: -2.74 to -1.38, P < 0.001), 12 h (MD = -1.72, 95%CI: -2.30 to -1.14, P < 0.001) and 24 h (MD = -1.03, 95%CI: -1.55 to -0.52, P < 0.001), respectively. Moreover, SAPB conferred a fewer postoperative opioid consumption (MD = -7.3 mg of intravenous morphine equivalent, 95%CI: -10.16 to -4.44, P < 0.001) and lower incidence of PONV (RR = 0.56, 95%CI: 0.41 to 0.77, P < 0.001). There was no difference between both groups regarding length of hospital stay and risk of dizziness.
Conclusion: SAPB shows an excellent performance in postoperative pain management in patients undergoing VATS by reducing pains scores, postoperative opioid consumption and incidence of PONV. However, due to huge heterogeneity, more well-designed, large-scale RCTs are needed to verify these findings in the future.
Keywords: Analgesia; Meta-analysis; Postoperative pain scores; Serratus anterior plane block; Video-assisted thoracoscopic surgery.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Comparison of the postoperative analgesic efficacy of serratus anterior plane block with different types of blocks for video-assisted thoracoscopic surgery: A systematic review and meta-analysis of randomized controlled trials.Turk Gogus Kalp Damar Cerrahisi Derg. 2024 Oct 30;32(4):419-435. doi: 10.5606/tgkdc.dergisi.2024.26887. eCollection 2024 Oct. Turk Gogus Kalp Damar Cerrahisi Derg. 2024. PMID: 39651044 Free PMC article.
-
A comparison of regional anesthesia techniques in patients undergoing video-assisted thoracic surgery: A network meta-analysis.Int J Surg. 2022 Sep;105:106840. doi: 10.1016/j.ijsu.2022.106840. Epub 2022 Aug 24. Int J Surg. 2022. PMID: 36030040 Review.
-
Serratus anterior plane block for video-assisted thoracoscopic surgery: A meta-analysis of randomised controlled trials.Eur J Anaesthesiol. 2021 Feb 1;38(2):106-114. doi: 10.1097/EJA.0000000000001290. Eur J Anaesthesiol. 2021. PMID: 32833856
-
Postoperative Analgesic Effects of Serratus Anterior Plane Block for Thoracic and Breast Surgery: A Meta-analysis of Randomized Controlled Trials.Pain Physician. 2023 Mar;26(2):E51-E62. Pain Physician. 2023. PMID: 36988359
-
Postoperative analgesic effects of paravertebral block versus erector spinae plane block for thoracic and breast surgery: A meta-analysis.PLoS One. 2021 Aug 25;16(8):e0256611. doi: 10.1371/journal.pone.0256611. eCollection 2021. PLoS One. 2021. PMID: 34432822 Free PMC article.
Cited by
-
Serratus Anterior Plane Block for Pain Management After Video-Assisted Thoracoscopic Surgeries: A Narrative Review.Medicina (Kaunas). 2025 May 28;61(6):1010. doi: 10.3390/medicina61061010. Medicina (Kaunas). 2025. PMID: 40572697 Free PMC article. Review.
-
Recent Advances in Perioperative Analgesia in Thoracic Surgery: A Narrative Review.J Clin Med. 2024 Dec 25;14(1):38. doi: 10.3390/jcm14010038. J Clin Med. 2024. PMID: 39797121 Free PMC article. Review.
-
Comparison of the postoperative analgesic efficacy of serratus anterior plane block with different types of blocks for video-assisted thoracoscopic surgery: A systematic review and meta-analysis of randomized controlled trials.Turk Gogus Kalp Damar Cerrahisi Derg. 2024 Oct 30;32(4):419-435. doi: 10.5606/tgkdc.dergisi.2024.26887. eCollection 2024 Oct. Turk Gogus Kalp Damar Cerrahisi Derg. 2024. PMID: 39651044 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
