

Central nervous system manifestations of LRBA deficiency: case report of two siblings and literature review
- PMID: 37443020
- PMCID: PMC10339488
- DOI: 10.1186/s12887-023-04182-z
Central nervous system manifestations of LRBA deficiency: case report of two siblings and literature review
Abstract
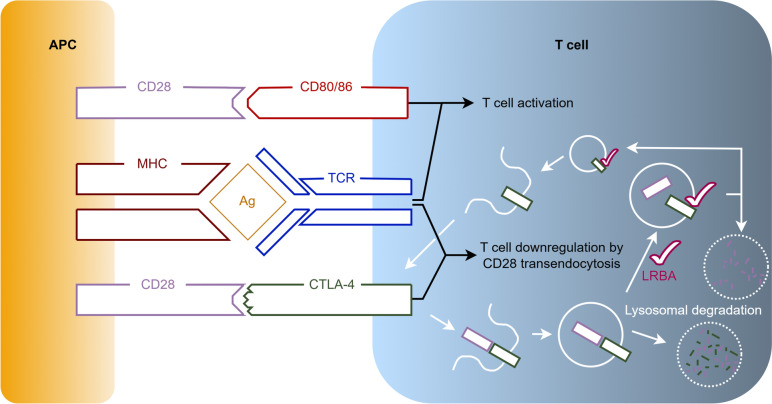
Background: LPS-responsive beige-like anchor protein (LRBA) deficiency is a primary immunodeficiency disease (PID) characterized by a regulatory T cell defect resulting in immune dysregulation and autoimmunity. We present two siblings born to consanguineous parents of North African descent with LRBA deficiency and central nervous system (CNS) manifestations. As no concise overview of these manifestations is available in literature, we compared our patient's presentation with a reviewed synthesis of the available literature.
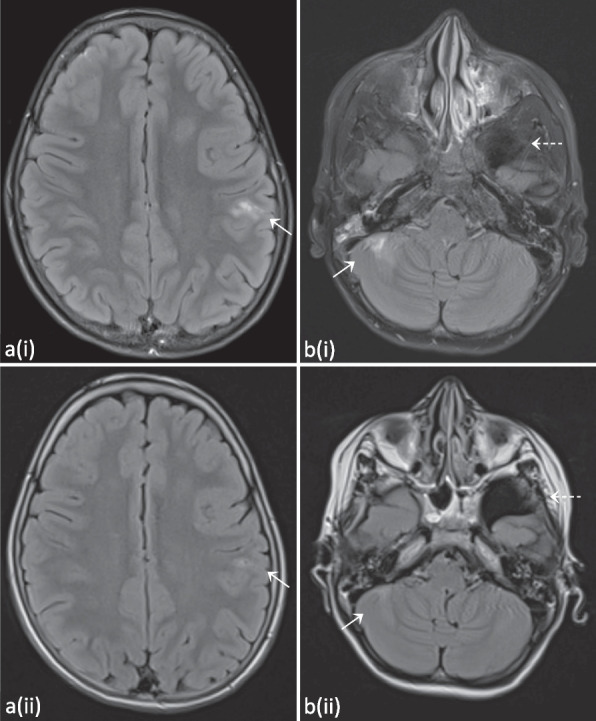
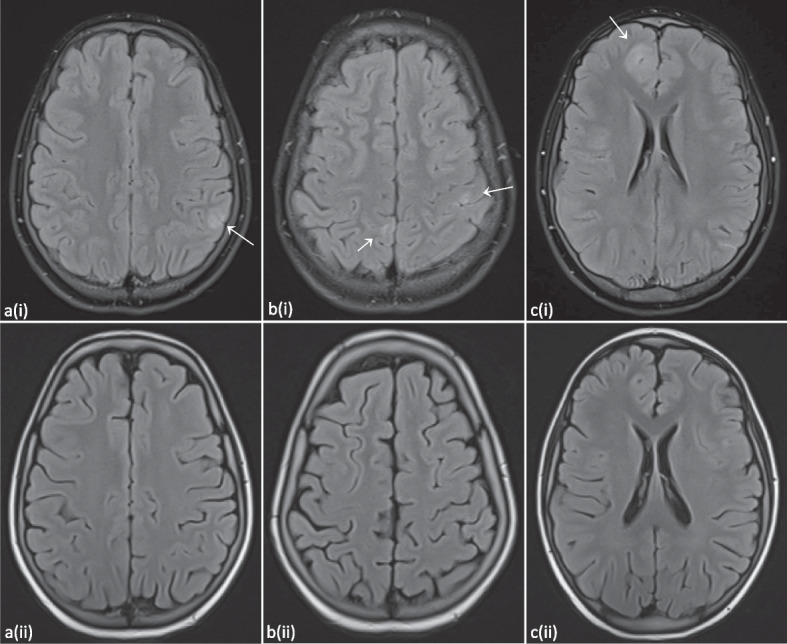
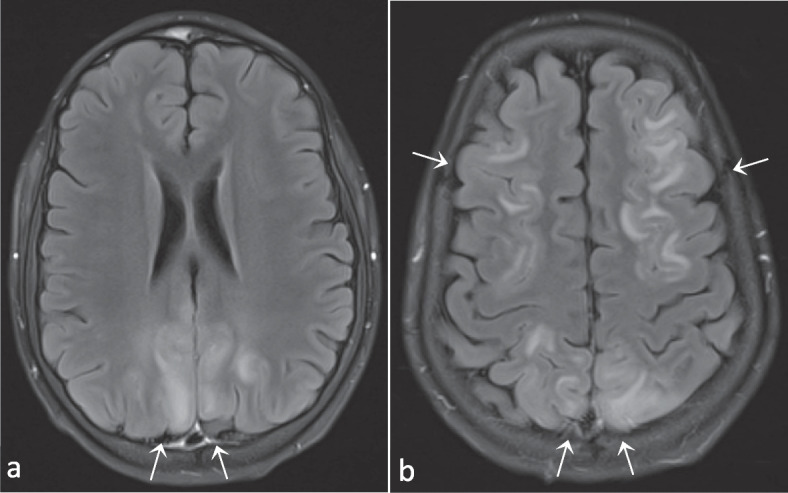
Case presentations: The younger brother presented with enteropathy at age 1.5 years, and subsequently developed Evans syndrome and diabetes mellitus. These autoimmune manifestations led to the genetic diagnosis of LRBA deficiency through whole exome sequencing with PID gene panel. At 11 years old, he had two tonic-clonic seizures. Brain MRI showed multiple FLAIR-hyperintense lesions and a T2-hyperintense lesion of the cervical medulla. His sister presented with immune cytopenia at age 9 years, and developed diffuse lymphadenopathy and interstitial lung disease. Genetic testing confirmed the same mutation as her brother. At age 13 years, a brain MRI showed multiple T2-FLAIR-hyperintense lesions. She received an allogeneic hematopoietic stem cell transplantation (allo-HSCT) 3 months later. Follow-up MRI showed regression of these lesions.
Conclusions: Neurological disease is documented in up to 25% of patients with LRBA deficiency. Manifestations range from cerebral granulomas to acute disseminating encephalomyelitis, but detailed descriptions of neurological and imaging phenotypes are lacking. LRBA deficiency amongst other PIDs should be part of the differential diagnosis in patients with inflammatory brain lesions. We strongly advocate for a more detailed description of CNS manifestations in patients with LRBA deficiency, when possible with MR imaging. This will aid clinical decision concerning both anti-infectious and anti-inflammatory therapy and in considering the indication for allo-HSCT.
Keywords: Case report; Central nervous system; Hearing loss; LRBA deficiency; MRI; Neurological.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Reiser M, Li K, Lockey RF, Wang J-W. Lipopolysaccharide Responsive Beige-Like Anchor Subcellular Localization Involving in Vesicle Trafficking Responsive to Lipopolysaccharide. Austin J Clin Immunol. 2014;1:1020.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
